|
[#1]
To reiterate:
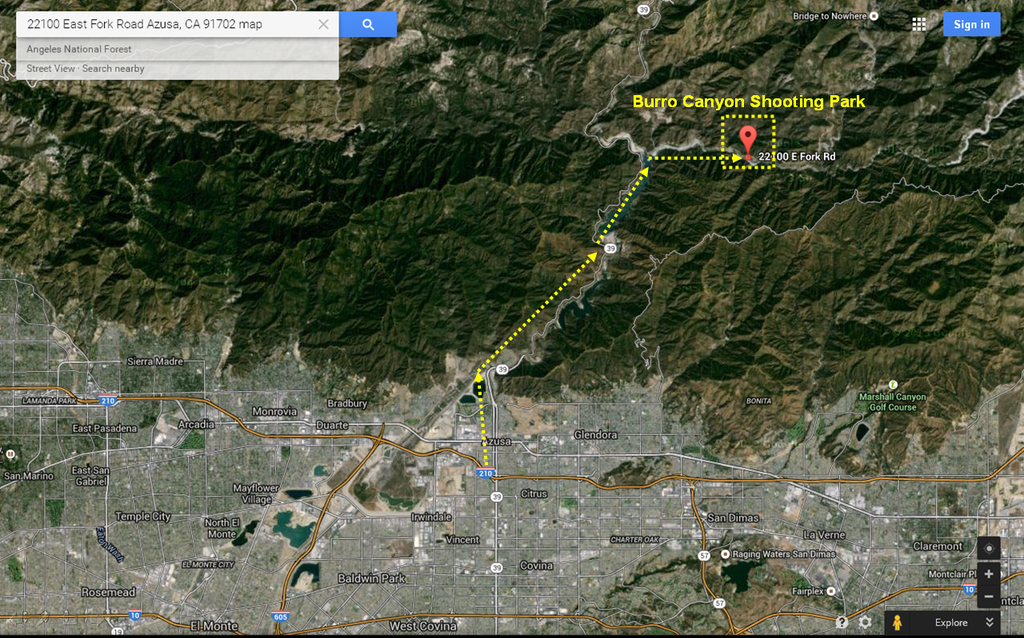
*Type of holster, carry etc. irrelevant to me as I was a first responder not the patients trainer. *Reason for private movement vs ambulance: Range is on top of a mountain 30 minutes from town. Ambulance = 1 hour round trip. *All trainers and RSOs should have a GSW kit either on them or centralized. *MEDEVAC plan should be briefed in bleeding detail, the range/class/group "medic" needs to be there from start to finish, no exceptions. |
|
|
|
[#2]
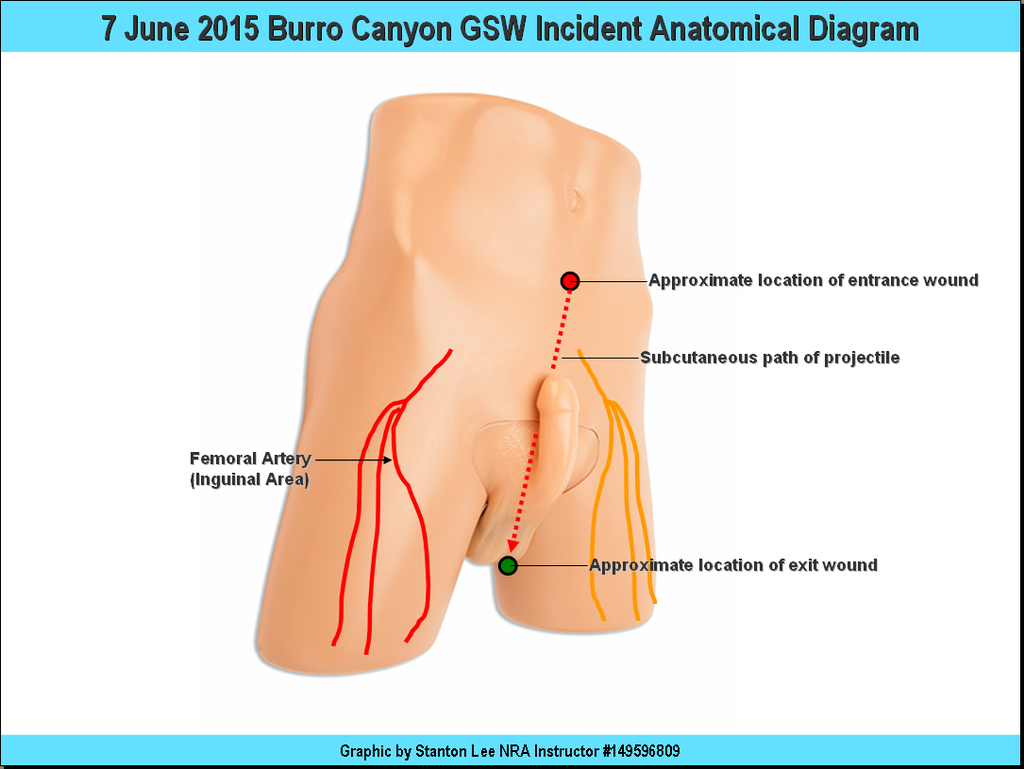
Quoted: To reiterate: *Type of holster, carry etc. irrelevant to me as I was a first responder not the patients trainer. *Reason for private movement vs ambulance: Range is on top of a mountain 30 minutes from town. Ambulance = 1 hour round trip. *All trainers and RSOs should have a GSW kit either on them or centralized. *MEDEVAC plan should be briefed in bleeding detail, the range/class/group "medic" needs to be there from start to finish, no exceptions. There also isn't good if any cell phone coverage there (in a valley) so just getting help is going to the ranger station or climbing up the hill (in car or on foot) to make a connection. I carry an Israeli bandage as well as a basic med kit. (No quick clot though.) ========== You didn't see a holster or hear about what he was doing to shoot himself? |
|
|
|
[#3]
Good on you, but calling off EMS was probably dumb. I worked that area for many years. Now, if the patient made the call to go on his own, and you have witnesses, then ignore the rest.
AMR (do they still have the contract?) could have met him with LA Co. FD coming off the access road. Mercy Air migt have flown there direct amd got him out sooner. Where the heck did his friends take him? There is a reason that we have trauma centers in SoCal. Did he go to Huntington Memorial (20 minutrs from the freeway, without traffic), or some other little ER along the way that had one doc, three nurses, no on call surgeon? Your "patient" bleeds out on the drive down. His friends say "well the paramedic said to drive him..." Any actual level of training is suddenly irrelevant when the police come to talk to you. If you truly have no stamdardized medical training you may be off the hook, but if you do, then you may have to worry about patient abandonment issues. |
|
|
|
[#4]
He got off light. Good job reacting, and addressing those wounds. Having a evac plan is now one of my musts.
Good write up. |
|
|
|
[#5]
Your kit is kind-of light. I suggest buying one of the more complete Larue or CavArms kits and supplementing it.
One pair of gloves is not enough and there are good ones and bad ones. You need the needle resistant 4 mil gloves, several pairs. One set for you, one for the first one that rips, and one set for a helper. Celox bandages and applicators. Think "blow out" kit. The Larue kit comes with a tourniquet that can be applied with one hand. This could end up being very important. I also added regular bandages, several kinds of tape, lip balm, sun screen, insect antihistamines, and a bunch of other items that slip my mind. I keep this kit in my truck and try to put it in any vehicle I am taking on a trip or to the range. |
|
|
|
[#6]
Quoted: Your kit is kind-of light. I suggest buying one of the more complete Larue or CavArms kits and supplementing it. One pair of gloves is not enough and there are good ones and bad ones. You need the needle resistant 4 mil gloves, several pairs. One set for you, one for the first one that rips, and one set for a helper. Celox bandages and applicators. Think "blow out" kit. The Larue kit comes with a tourniquet that can be applied with one hand. This could end up being very important. I also added regular bandages, several kinds of tape, lip balm, sun screen, insect antihistamines, and a bunch of other items that slip my mind. I keep this kit in my truck and try to put it in any vehicle I am taking on a trip or to the range. We're talking about two different things; a GSW kit which ideally should be on you at all times at the range and a general purpose first aid kit.
The misc stuff like lip balm, sun screen etc. do not belong in a GSW kit and can go in your general first aid kit. I also have a general/community FAK bag centralized that duplicates and exceeds the same capabilities. Also, you do realize that the great majority of trainers, groups, dudes "shoot'n shit" on any given weekend at the range probably have some band aids and tape as their first aid kit (if anything at all)? Most probably don't have a MEDEVAC plan. |
|
|
|
[#7]
Quoted: Good on you, but calling off EMS was probably dumb. I worked that area for many years. Now, if the patient made the call to go on his own, and you have witnesses, then ignore the rest. Range management was in 100% agreement with my actions. AMR (do they still have the contract?) could have met him with LA Co. FD coming off the access road. Yes, could have done this, should have been in their party's plan). Mercy Air migt have flown there direct amd got him out sooner. Range management says anywhere from 15-45 minutes and is a large logistical footprint. Depends on where Air5 is that time. Where the heck did his friends take him? There is a reason that we have trauma centers in SoCal. Did he go to Huntington Memorial (20 minutrs from the freeway, without traffic), or some other little ER along the way that had one doc, three nurses, no on call surgeon? Your "patient" bleeds out on the drive down. His friends say "well the paramedic said to drive him..." Any actual level of training is suddenly irrelevant when the police come to talk to you. If you truly have no stamdardized medical training you may be off the hook, but if you do, then you may have to worry about patient abandonment issues. OK, in the time we wait for an ambulance the patient can bleed out and die as well. Also, to avoid legal entanglements I could have just as easily crossed my arms and said "too bad for him" and let his friends figure something out. He could have died and then rose from the grave. So I don't get the "what if ing". A lot of things could have happened but he lived and was released from the hospital the next day. Quoted: Good on you, but calling off EMS was probably dumb. I worked that area for many years. Now, if the patient made the call to go on his own, and you have witnesses, then ignore the rest. Range management was in 100% agreement with my actions. AMR (do they still have the contract?) could have met him with LA Co. FD coming off the access road. Yes, could have done this, should have been in their party's plan). Mercy Air migt have flown there direct amd got him out sooner. Range management says anywhere from 15-45 minutes and is a large logistical footprint. Depends on where Air5 is that time. Where the heck did his friends take him? There is a reason that we have trauma centers in SoCal. Did he go to Huntington Memorial (20 minutrs from the freeway, without traffic), or some other little ER along the way that had one doc, three nurses, no on call surgeon? Your "patient" bleeds out on the drive down. His friends say "well the paramedic said to drive him..." Any actual level of training is suddenly irrelevant when the police come to talk to you. If you truly have no stamdardized medical training you may be off the hook, but if you do, then you may have to worry about patient abandonment issues. OK, in the time we wait for an ambulance the patient can bleed out and die as well. Also, to avoid legal entanglements I could have just as easily crossed my arms and said "too bad for him" and let his friends figure something out. He could have died and then rose from the grave. So I don't get the "what if ing". A lot of things could have happened but he lived and was released from the hospital the next day. |
|
|
|
[#8]
As said before, you did abandon the patient. You should have rode with him. Once you put hands on and start care you are committed to the patient until they die, you are too physically exhausted to continue (CPR), or someone with equal or higher training relieves you. Best option would have been to call EMS and meet them in route. I would add some compressed gauze to your kit for areas that cannot be addressed with an Israeli. Good on you for responding though.
|
|
|
|
[#9]
100% success in my opinion.
|
|
|
|
[#10]
Good for you in stepping up... my thoughts on calling EMS... why not? At least the wheels could be in motion... the car used to transport the patient could have got a flat tire, took a shit, or the driver could have had an accident/or got stuck (due to being excited, scared, or in too big a hurry). It's better to have things in motion than trying to get them in motion later. Again, good on you for stepping up... thanks for the AAR.
At my place... the grid coordinates are posted in the class, GSW kit is on hand, and two students are pre-identified to respond to the gate to flag/direct EMS in (if one of these students are the subject injured, the other grabs the first person they see)... all this is covered BEFORE and DURING class and is part of the emergency response plan. I send two students to the entrance just in case multiple EMS units respond. |
|
|
|
[#11]
Probably would have gone with the patient, but everything else there seems objectively medically reasonable.
|
|
|
 Win a FREE Membership!
Win a FREE Membership!
Sign up for the ARFCOM weekly newsletter and be entered to win a free ARFCOM membership. One new winner* is announced every week!
You will receive an email every Friday morning featuring the latest chatter from the hottest topics, breaking news surrounding legislation, as well as exclusive deals only available to ARFCOM email subscribers.

AR15.COM is the world's largest firearm community and is a gathering place for firearm enthusiasts of all types.
From hunters and military members, to competition shooters and general firearm enthusiasts, we welcome anyone who values and respects the way of the firearm.

Subscribe to our monthly Newsletter to receive firearm news, product discounts from your favorite Industry Partners, and more.
Copyright © 1996-2024 AR15.COM LLC. All Rights Reserved.
Any use of this content without express written consent is prohibited.
AR15.Com reserves the right to overwrite or replace any affiliate, commercial, or monetizable links, posted by users, with our own.