GA, USA
|
Posted: 3/9/2016 10:25:16 PM EDT
[Last Edit: GypsyDoc]
Just checking… I have a CRAZY 12 lead I'd like to post if anyone is interested. If so, give me a day or so.
|
|
|
|
[#1]
I'm going to regret this, but post it up

|
|
|
|
|
[#2]
Originally Posted By TNBayou:
I'm going to regret this, but post it up Oi, me too. Was never my strongest skill. JEMS posts them up on FB from time to time but that's about the only ones I see these days. |
|
|
|
|
[#3]
I suck, so I need this thread.
oh, and in before Dale Dubin the PedoPhile |
|
|
|
|
[#4]
Post it up.
|
|
|
|
GA, USA
|
[Last Edit: GypsyDoc]
[#5]
Hi guys
Thanks for your patience. A little background... I work overseas at a small hospital providing medical services for American Expats and foreign nationals. This gentleman was a 48yo male who came to the walk-in clinic c/o RIGHT neck and shoulder pain with SOB, his neck pain increased upon palpation. He was tachycardic, increased WOB, slightly hypertensive and O2 sat around 91-92% on room air. He was observed to have this ECG. We have NO cardiologist on staff, just an ER physician, Surgeon, two PA's and a CRNA... of course a few nurses and some paramedics. The decision was made to have him MedEvac'ed out so he was "admitted" overnight until arrangements are finalized. The only thing abnormal from his labs were increased white count around 12.5 and a glucose level of about 160... cardiac enzymes are negative. 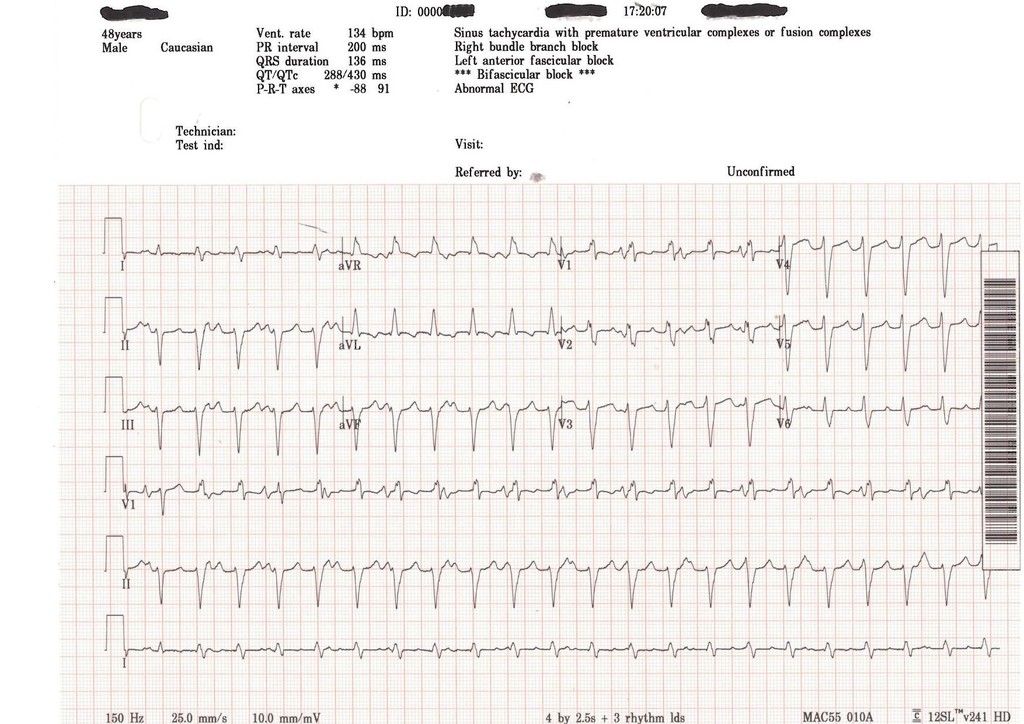
|
|
|
PA, USA
|
[#6]
That look like cardiac damage from a previous issue to me. And the increase of pain upon palpation kinda sound like something else is going on
|
|
|
|
[#7]
Originally Posted By EvanWilliams:
I suck, so I need this thread. oh, and in before Dale Dubin the PedoPhile LoL yea but his orange book was quite good |
|
|
|
|
[Last Edit: AGW]
[#8]
PE is high on the list, no slam dunk right heart strain/S1Q3T3 though.
No ST elevation, so unlikely an MI in the setting of negative trops (if you use high sensitivity assays), Unlikely to be pericarditis. No alternans, pseudo Wenkebach in some of the leads... Did O2 improve his sats? CXR? Fluid overloaded, acute (on chronic) CHF? Does he have a cardiac history? Was there a differential of his white count? BNP? |
|
|
|
GA, USA
|
[Last Edit: GypsyDoc]
[#9]
Initial thought was a PE. He received fluids but never had any urine output through the night. He was working the breathe with a RR 30-32, no improvement of sats. The ER doc was racking his brain trying to figure out what was going on.
Looking at the potential RBBB in V1 with Slight ST depression, I was thinking posterior MI along with some type of AV dissociation. I came in early just to see what was going on and the pt looked like crap. I listened him and he was wet with slight audible rhonchi and worsening sats. I suggested CPAP and the doc said sure. Sats came back up to high 80's/low 90's. The CRNA came in a couple hours later with our surgeon and decided to intubate him. Lung compliance was good but could never get sats out of the low 90's and pressure becomes unstable. An hour later he arrest. |
|
|
|
[Last Edit: Sartorius]
[#10]
1. First degree block
2. Inverted T-waves in AvL, hard to say about I. 3. Almost no R-wave progression to speak of in the precordial leads 4. RBBB with LAFB (noted by the computer) 5. Wide QRS (greater than 100-120 ms) 6. Significantly negative axis 7. Not sure about the PVC or Fusion Beats At least it's sinus rhythm and doesn't have tombstones in the ST segment. That's about all that you can say that's good about it. Did this guy have a D-Dimer or BNP? CXR? So what's everyone's different dx on this? -PE -Hypertensive cardiomyopathy -Ischemic cardiomyopathy (with that axis, an LAD lesion is possible) -Prior "silent" MI -Hypertensive cardiomyopathy Do you know what they found with him? I think a MedEvac was a very good idea, speaking as a dumb ER and Urgent Care doc. He needs an echo. ETA: I just saw your newest post, 7 seconds before mine. ETA2: Can you get a CT where you're working? What about a dissecting thoracic aneurysm? |
|
|
|
GA, USA
|
[Last Edit: GypsyDoc]
[#11]
Unable to obtain a good patient history as he was a foreign national. No CT available and our Rad Tech for the portable X-ray was entering the country coming off of R&R status.
D-Dimer negative. He went into PEA four times over the course of about 6 hours and was successfully resuscitated. I will post some other 12 Leads later with more info. |
|
|
|
[Last Edit: AGW]
[#12]
No improvement in his sats with O2 and NIPPV suggests some kind of shunt, and wetness + htn suggests some fluid overload. I agree he needs ultrasound in his life (needed...?). Was there ever a chest x-ray? I don't know if I would have given him fluids with his presentation but I suppose it called his kidney function into question, so diuresis could have been tough. Did he have a blood gas? Pre vs post intubation? What precipitated his arrest (RSI?)? Also, was a carcinogenic arrest or hypoxic/apneic arrest? What rhythm?
ETA: I see PEA now. PEA tends to follow hypoxemia, so this guy definitely has some gas exchange issues that can't keep up with myocardial demand. |
|
|
|
|
[#13]
With PEA, what about the H's and T's?
Hypovolemia Hypoxia Hydrogen ion (acidosis) Hyper/Hypo-kalemia Toxins Tamponade (no trauma, but maybe a contained dissection?) Tension pneumo (probably not) Thrombosis (but a negative D-dimer?) CMP? What were his kidneys, K and CO2 showing? Do you have an iStat there? Tox screen, even a urine dipstick/cup tox? I love these cases. How am I supposed to sleep now? And stupid daylight savings is coming this weekend.  |
|
|
|
|
[#14]
I know, right? What's his nationality? Any travel history, sick contacts, you could glean? Rashes or anything?
Hell, just send to the cath lab. |
|
|
|
|
[Last Edit: Sartorius]
[#15]
Originally Posted By AGW: I know, right? What's his nationality? Any travel history, sick contacts, you could glean? Rashes or anything? Hell, just send to the cath lab. And as AGW's northern neighbor, I really wish Utah could figure out the Arizona plan and stop with the time changes. It's not like most of us are out bringing in the crop this weekend. |
|
|
|
GA, USA
|
[#16]
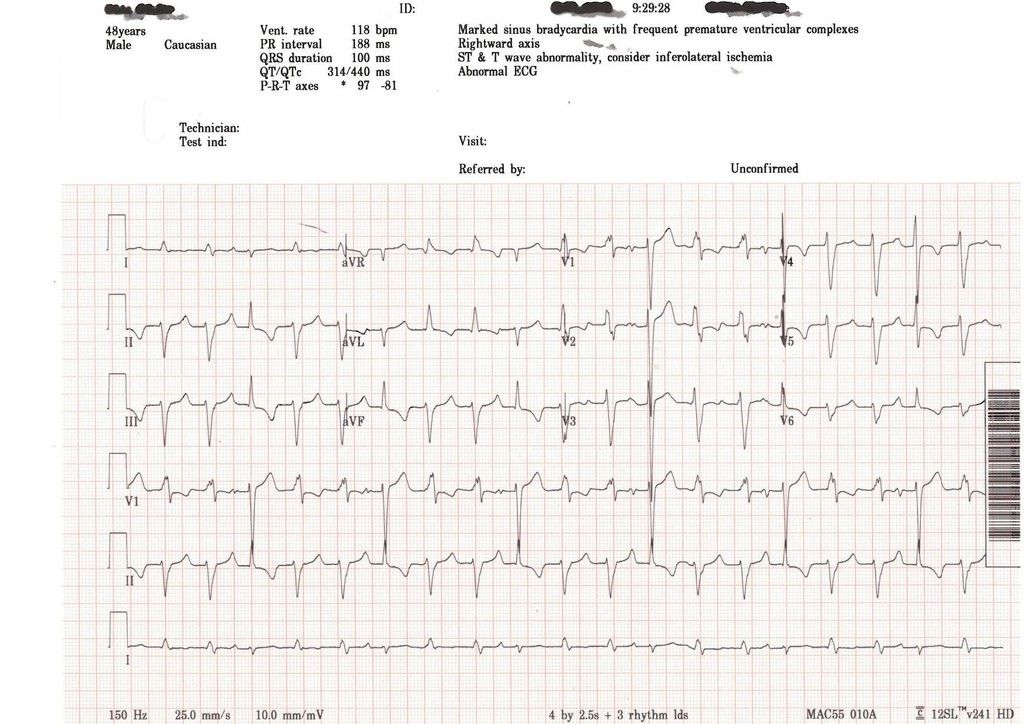
Here is an ECG between one of his PEA episodes; a trigeminal rhythm.
|
|
|
GA, USA
|
[#17]
All I can say is he is of Eastern European descent, and a normally healthy looking male.
Cardiac Enzymes and D-Dimer continued to be negative to this point. Our Lab guy even ran controls just to make sure his machines were functioning properly. ER Doc was stuck on diagnoses of Myocarditis. His rationale was that the right neck pain could have been from inflammation of the right carotid artery, coming off the brachiocephalic branch of the aorta, and similar ECG findings during his research. Also his white count went from 12.5 to 22, but he was afebrile. Before he was tubed, a foley was put in and they got around 400cc of clear urine. I am not sure of all the meds the CRNA used for RSI, but I know she used Rocuronium, possibly versed and fentanyl. No Succ. We have a portable sonogram and one of the docs took a quick look at the patients heart and saw no pericardial fluid. No pneumothorax noted or suspected Lab Chemistry I cannot remember specifically. But I do know his K+ was low normal. And a negative on the ABG's. |
|
|
GA, USA
|
[Last Edit: GypsyDoc]
[#18]
It was a pain trying to maintain his pressure. He would be good one minute and drop the next. He finally leveled out with an Isoproterenol drip. Before that he was on an Amiodarone and neosynephrine.
He converted to sinus rhythm and maintained it for a while; note the ST depression in the inferior and lateral leads: I mean... WTF was going on with this guy!! 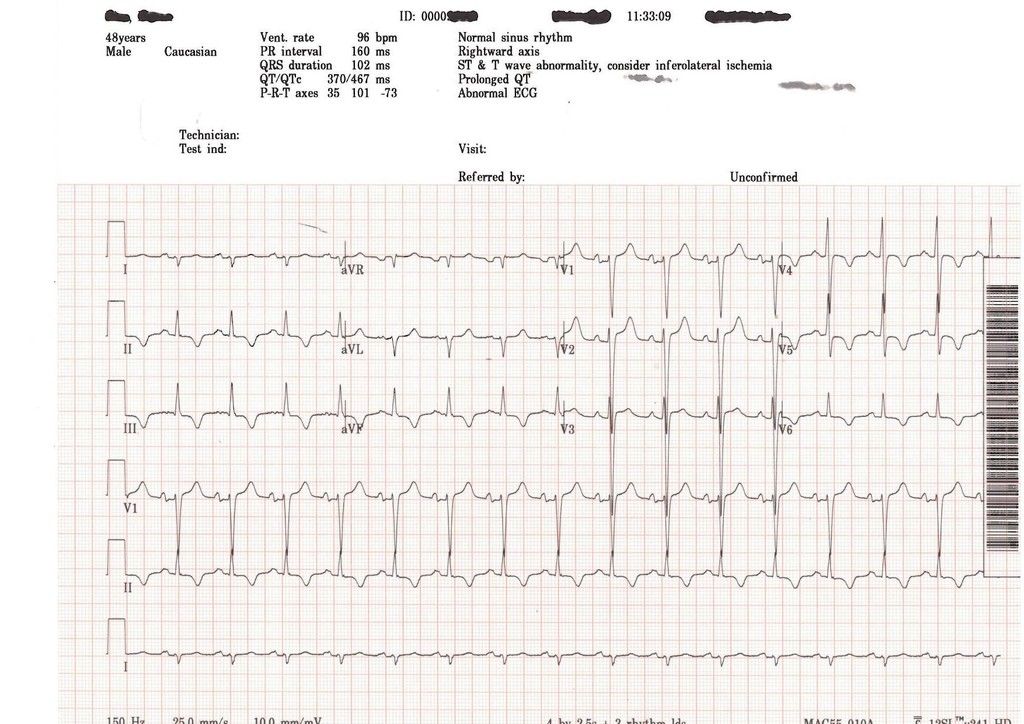
|
|
|
|
[#19]
Cor pulmonale is a little bit more visible in this ecg but still no S1. The st and t wave depressions could be post-arrest changes. I've seen a case where a blown valve looks all sorts of weird and can't really be seen or heard without a formal echo. I keep going back to his shunt - hypertensive with congested lungs, but a moderate amount of clear urine no longer concerns me for overload as much. He's obviously got a weaker heart for such an extreme axis, and he appears to be trying to overcome some high vascular resistance, more systemic than pulmonary.
What exactly were his pre-intervention pressures? Physical exam-wise, any edema or murmurs? |
|
|
|
GA, USA
|
[#20]
Prior to this thing kicking off, his pressures were 140-150/100ish. Following intubation, 70-80/50ish. No edema or murmurs were noted on PE.
|
|
|
|
[#21]
I sent this in a PM to GypsyDoc and he didn't laugh me off the internet, so I thought I'd post it up here to see if anyone else wants to chime in...
Ok, I've been debating whether or not to expose myself to potential ridicule here for the last few days, but what the heck, here we go. Bear in mind I am a lowly little paramedic student, so I'll just be over here in my glass house not throwing any big stones I didn't have the guts to post in the thread so you're stuck with an IM I am seeing 3rd degree junctional in that first strip in addition to the RBBB. I see extra p-waves in Lead I and they do not appear to have any correlation to the (narrow) QRS complexes. We have been taught to drop into V1 first, and it looks like there are embedded p-waves there as well. Am I just seeing things that aren't really there? Wouldn't 3J and a RBBB correspond with the symptoms the PT was experiencing as well as not responding to the amiodorone drip? It's a shame we don't know if the RBBB is new onset or not, that could have helped you out tremedously. 12 leads are far and away my weakest area so I am trying to take every opportunity to learn that I can get. Please don't mistake this as second guessing your actions; it is 12 lead interpretation afterall |
|
|
|
|
[Last Edit: TNBayou]
[#22]
Also, a long shot here, but how were his teeth? We recently had a PT in the ED who presented in a similar manner (we could not get their sats up no matter how much O2 we gave). Turns out they had a sensitivity to 'caine' drugs. Our PT had been taking orajel and had an unknown sensitivity to it. There was oxygen on their hemoglobin but the meds were preventing the body from being able to utilize it. Wouldn't necessarily be caused by orajel but a similar med could do it. Treatment for it was Methyl Blue.
ETA: I may have missed where you ran the appropriate labs that would have identified this. We caught it because their PAO2 was over 300 but they were still sating in the 70's and 80's. |
|
|
|
GA, USA
|
[#23]
Originally Posted By TNBayou:
Also, a long shot here, but how were his teeth? We recently had a PT in the ED who presented in a similar manner (we could not get their sats up no matter how much O2 we gave). Turns out they had a sensitivity to 'caine' drugs. Our PT had been taking orajel and had an unknown sensitivity to it. There was oxygen on their hemoglobin but the meds were preventing the body from being able to utilize it. Wouldn't necessarily be caused by orajel but a similar med could do it. Treatment for it was Methyl Blue. ETA: I may have missed where you ran the appropriate labs that would have identified this. We caught it because their PAO2 was over 300 but they were still sating in the 70's and 80's. Interesting theory, but I am not sure how "caine" drugs would affect the transfer of O2 to or from hemoglobin. Most "caine" drugs act a Na+ channel blockers, thereby inhibiting depolarization of the cellular membrane. O2 binds to hemoglobin through a process of coopertivity (SP?)... as one O2 molecule binds to hemoglobin it increases the affinity of the next O2 molecule to bind, the second O2 molecule then increases affinity for the 3rd O2 molecule and so forth. CO2 and O2 then transfer (diffuse) to and from tissue-vessel due to pressure and concentration gradient differences. So I am curious how this would affect arterial PO2... interesting! Who'd a thunk you could have so much fun talking medical crap on a gun website!! |
|
|
|
[Last Edit: TNBayou]
[#24]
I have to admit, I never expected this kind of discussion here either!
We actually attended an airway lecture during one class given by the head of Vanderbilt's Respiratory department and he mentioned the methemoglobinemia. At the time I thought "I'll never remember that, it's way too rare, I'll never see it" and promptly forgot. About 2 weeks later, it comes across the ED I was doing a clinical in. I'd like to say I remembered and caught it, but that would be a lie . It's also worth noting that the ED doc caught it fairly quickly due to the fact that he had seen it once before. He said the first time didn't go so quickly and took a fair bit of research to figure out!
I'd also like to say that I'm spouting this next part from memory, but, well, you know Introduction Methemoglobinemia is a rare cause of hypoxemia, characterized by abnormal levels of oxidized hemoglobin that cannot bind to and transport oxygen. Case presentation A 62-year-old male underwent bronchoscopy where lidocaine oral solution and Hurricaine spray (20% benzocaine) were used. He developed central cyanosis and his oxygen saturation was 85% via pulse oximetry. An arterial blood gas revealed pH 7.45, PCO2 42, PO2 282, oxygen saturation 85%. Co-oximetry performed revealed a methemoglobin level of 17.5% (normal 0.6–2.5%). The patient was continued on 15 L/minute nonrebreathing face mask and subsequent oxygen saturation improved to 92% within two hours. With hemodynamic stability and improved SpO2, treatment with methylene blue was withheld. Conclusion Methemoglobinemia is a potentially lethal condition after exposure to routinely used drugs. Physicians should be aware of this complication for early diagnosis and treatment. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2263062/ Also (emphasis mine): Physical findings may include the following:
• Discoloration of the skin and blood (the most striking physical finding) • Cyanosis – This occurs in the presence of 1.5 g/dL of methemoglobin (as compared with 5 g/dL of deoxygenated hemoglobin) • Seizures • Coma • Dysrhythmia (eg, bradyarrhythmia or ventricular dysrhythmia) • Acidosis • Cardiac or neurologic ischemia • Pallor of the skin or conjunctiva (suggestive of anemia and possible hemolysis) • Skeletal abnormalities and mental retardation Treatment modalities include the following:
• Methylene blue – This is the primary emergency treatment for documented symptomatic methemoglobinemia (contraindicated in G6PD deficiency and ineffective with hemoglobin M) http://emedicine.medscape.com/article/204178-overview The head of the pharmacy personally delivered the methyl blue due to 'abnormal' dosage ordered. He wanted to make sure we ordered correctly and see the situation first hand. It worked relatively quickly and IIRC we discharged the PT. Those were two quick links that popped up on google, there's plenty more out there. I'm still not convinced it fits all the criteria of what your guy had, but I would have loved to see what his PaO2 was! The neck pain is a bit of an outlier, as well as the fluids, but nothing says he didn't have some comorbidities. Also, I ran the 12 leads past the rest of the class. So far everyone in my class that has replied has called the first one as a 3rd degree block (not surprising since we all learned to read them the same way haha). I'll be back in class tomorrow and I'll try and see what the head of the program thinks. He is an ECG 'Guru', so it should be interesting. |
|
|
|
GA, USA
|
[Last Edit: GypsyDoc]
[#25]
Awesome! I read the article, very cool! Now I need to find out how this stuff converts at the biochemical/cellular level.
|
|
|
|
[#26]
I have nothing really useful to add, my only exposure was to a 3-wire in Physiology lab, but even I could tell there was something extremely wrong with that.
|
|
|
|
|
[#27]
The consensus from my class was 3*I, but again, not surprising since we all learned from the same set of rules. I also sent it to the medical officer for my agency and got this back :
Took a look at the EKG and related medical problems. My initial thought is that the EKG changes are the result of something that is not cardiac in nature. Who goes into cardiac arrest due to a RBBB and possible 3rd degree block that is relatively fast??
Lead AvR should be negatively deflected in the first strip but is not, why? Dextrocardia?? NO WAY?? Pulmonary embolus?? Maybe?? The SOB and declining sats leads back to a potential cardiac issue. When we get together we should sit down and hash this one out. Confounding and confusing. A good teaching/learning scenario. We should talk about this at the upcoming ACLS classes in April. Did you ever get any update on the guy? |
|
|
|
GA, USA
|
[Last Edit: GypsyDoc]
[#28]
Yes, I received an update the other day… The guy just got extubated and is receiving, or has received, some type of ventricular pump. I will have to ask Monday for more details.
I am interested to hear what else your medical officer says. |
|
|
|
[Last Edit: Azygos]
[#29]
Originally Posted By GypsyDoc:
Yes, I received an update the other day… The guy just got extubated and is receiving, or has received, some type of ventricular pump. I will have to ask Monday for more details. I am interested to hear what else your medical officer says. Interesting. I was wondering if he boxed his LV and went into acute edema. It would make sense if he's getting an LVAD or Impella. The PEA instead of VF makes me scratch my head a bit, as do the funky rhythm changes. I have seen one case of presumed viral myocarditis that temporarily took out the conduction system (AV dissociation/3rd degree) of a marathon runner in her 20s. |
|
|
|
 Win a FREE Membership!
Win a FREE Membership!
Sign up for the ARFCOM weekly newsletter and be entered to win a free ARFCOM membership. One new winner* is announced every week!
You will receive an email every Friday morning featuring the latest chatter from the hottest topics, breaking news surrounding legislation, as well as exclusive deals only available to ARFCOM email subscribers.

AR15.COM is the world's largest firearm community and is a gathering place for firearm enthusiasts of all types.
From hunters and military members, to competition shooters and general firearm enthusiasts, we welcome anyone who values and respects the way of the firearm.

Subscribe to our monthly Newsletter to receive firearm news, product discounts from your favorite Industry Partners, and more.
Copyright © 1996-2024 AR15.COM LLC. All Rights Reserved.
Any use of this content without express written consent is prohibited.
AR15.Com reserves the right to overwrite or replace any affiliate, commercial, or monetizable links, posted by users, with our own.















