|
[#1]
Originally Posted By exponentialpi: There is and anyone disputing that is not credible. The question is how many would have been prevented if early action therapeutics were pushed instead of the full court press for vaccines. Some should head to the gallows for that. Originally Posted By exponentialpi: Originally Posted By exDefensorMilitas: Originally Posted By planemaker: Originally Posted By exDefensorMilitas: Originally Posted By exponentialpi: Originally Posted By exDefensorMilitas: Originally Posted By lorazepam: Originally Posted By 79CJ7: Millions more died last year and so far this year. Look up the excess mortality stats. The facts do not support your opinion. Lol, excess mortality. Even though I've been a Flubro since the beginning, there is indeed an increase over the yearly projected deaths in most of the demographic groups. That can't really be disputed. There has been. The question is did it shift timing (were a majority on the end of the mortality table already) or a real impact. We won’t know for a few years. I think the biggest confounding variable to evaluating the impact of the frontloading will be to adequately factor in the migration of people that move from one age demographic to the next. Theoretically, a glut or deficit in the raw number of people moving from a younger to an older demo, could either mask or exacerbate the "apparent" impact, while the underlying statistics tell the opposite story. Hopefully that makes sense.  The other thing about 2020 that was discussed previously was that as lockdowns, shutdowns, etc were implemented, people of all age groups simply stopped engaging in the types of activities that they used to do. Some of those were activities that carried risk, eg. driving - more work from home = less driving. It would be interesting to look at a time history to see as people got back to work, lockdowns/shutdowns etc. went away that those risks started increasing again. Bottom line to me is that I'm not convinced "excess mortality" stats are going to tell the whole story. The number is pulled in both directions, but there is excess mortality at the end of the day, due to SARS-CoV-2 There is and anyone disputing that is not credible. The question is how many would have been prevented if early action therapeutics were pushed instead of the full court press for vaccines. Some should head to the gallows for that. To be fair, Operation Warp Speed and the media both shortchanged monoclonal antibodies and fixated heavily on vaccines. Even if mcab's were pushed heavily, I'm not entirely sure if the necessary manufacturing capacity could have been spun up fast enough to make a difference early on. |
|
|
|
|
[#2]
bump to turn stuck page
|
|
|
|
|
[#3]
Originally Posted By 79CJ7: 740,000 Americans might disagree with you. If they were still around. Originally Posted By 79CJ7: Originally Posted By Gunner226: Unless I really take a turn for the worse, I'd put my personal experience in the "moderate cold" catagory, so far. I realize some aren't so lucky, but forcing a vaccine for this is BS. Especially a vaccine that is showing less and less efficacy - if it ever had any efficacy to begin with. This is certainly not the zombie apocalypse virus some of us thought it might turn out to be last January. 740,000 Americans might disagree with you. If they were still around. You still disinfect your mail, don’t you? |
|
|
|
|
[#4]
Originally Posted By fl-ar-fan: You still disinfect your mail, don’t you? Originally Posted By fl-ar-fan: Originally Posted By 79CJ7: Originally Posted By Gunner226: Unless I really take a turn for the worse, I'd put my personal experience in the "moderate cold" catagory, so far. I realize some aren't so lucky, but forcing a vaccine for this is BS. Especially a vaccine that is showing less and less efficacy - if it ever had any efficacy to begin with. This is certainly not the zombie apocalypse virus some of us thought it might turn out to be last January. 740,000 Americans might disagree with you. If they were still around. You still disinfect your mail, don’t you? A lot of them were riding motorcycles when they died of covid. |
|
|
|
|
[#5]
Originally Posted By FlashMan-7k: Ok, now THIS is attention getting: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1023849/Vaccine_surveillance_report_-_week_40.pdf From page 13 (numbered 12 on the pdf) ... Column labelled "Rates among persons vaccinated with 2 doses (per 100,000)" Negative efficacy vs catching the CCP crud, depending on your age group. Yep... think I'm gonna be watching next month's report to see if this isn't a blip...  ----- Ok, I give up, the stupid forum upload a jpg thing isn't working and won't tell me why. Managed a reverse search and found a copy on the net: https://westernrifleshooters.us/wp-content/uploads/2021/10/oops-uk-1024x555.png https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1027511/Vaccine-surveillance-report-week-42.pdf Interpretation of data These data should be considered in the context of vaccination status of the population groups shown in the rest of this report. The vaccination status of cases, inpatients and deaths is not the most appropriate method to assess vaccine effectiveness and there is a high risk of misinterpretation. Vaccine effectiveness has been formally estimated from a number of different sources and is described earlier in this report. In the context of very high vaccine coverage in the population, even with a highly effective vaccine, it is expected that a large proportion of cases, hospitalisations and deaths would occur in vaccinated individuals, simply because a larger proportion of the population are vaccinated than unvaccinated and no vaccine is 100% effective. This is especially true because vaccination has been prioritised in individuals who are more susceptible or more at risk of severe disease. Individuals in risk groups may also be more at risk of hospitalisation or death due to non- COVID-19 causes, and thus may be hospitalised or die with COVID-19 rather than because of COVID-19. The case rates in the vaccinated and unvaccinated populations are crude rates that do not take into account underlying statistical biases in the data. There are likely to be systematic differences in who chooses to be tested and the COVID risk of people who are vaccinated. These biases become more evident as more people are vaccinated and the differences between the vaccinated and unvaccinated population become systematically different in ways that are not accounted for without undertaken formal analysis of vaccine effectiveness as is made clear. NIMS is used as a denominator because it is a database of named individuals eligible for vaccination in which there is a record of each individual’s vaccination status. It stuck around for the next week. |
|
|
|
|
[#6]
Hnm
|
|
|
|
|
[#7]
|
|
|
|
CA, USA
|
[#8]
Originally Posted By exponentialpi: Welcome to 2021 gents. It keeps giving 2020 a run for it's money. https://www.ar15.com/media/mediaFiles/200878/RoundandRound_JPG-2142317.JPG 2021 has comprehensively kicked 2020's ass. And there's still 2 months to go ... |
|
|
|
[Last Edit: HighDesert6920]
[#9]
Originally Posted By fl-ar-fan: You still disinfect your mail, don't you? Originally Posted By fl-ar-fan: Originally Posted By 79CJ7: Originally Posted By Gunner226: Unless I really take a turn for the worse, I'd put my personal experience in the "moderate cold" catagory, so far. I realize some aren't so lucky, but forcing a vaccine for this is BS. Especially a vaccine that is showing less and less efficacy - if it ever had any efficacy to begin with. This is certainly not the zombie apocalypse virus some of us thought it might turn out to be last January. 740,000 Americans might disagree with you. If they were still around. You still disinfect your mail, don't you? A study from several years ago (long before the chinese virus) found feces on nearly 3/4 shopping carts. Look at the people in wally world next to you....they are wiping, picking, and licking all kinds of things....the fat hairy weirdo in line ahead of you is picking his nose, swiping his greasy hair back, farts and then reaches down to scratch his ass....then goes tap, tap, tap on the payment terminal....maybe sneezes in your direction...he was rummaging through all those bags of chips just before you picked out a bag. So his nasty crotch snot is smeared across the top of your chip bag....now you've got the munchies, and open the bag of chips, rubbing your hands through that guys snot, and then you grab a handful of chips and snarf them down....infected snot and all! What about those delicious apples you enjoy? Ever drive by an apple orchard during picking season? Of course, they're all illegals - but anyway, notice where the porta-potty units are - at the edge of the field...no hand washing stations to be seen....last night was chalupa night at Dos Gringos....makes Taco Bell look like quality...the guys in the field just went there last night for cheap beer and chalupas, now they have feel a power growler coming on right before picking shift. It's a mess in there! Unfortunately no hand washing stations...so just wipe hands on pants, and start picking fresh apples for the rich gringos. Now at the store, the apples are all coated with....something...something you're going to eat - because cleaning foods before eating is for pussy doomers! You're so brave! |
|
|
|
|
[#10]
Something to keep an eye out for:
|
|
|
|
|
[#11]
Originally Posted By FlashMan-7k: Something to keep an eye out for:
Thanks for sharing. The CDC is beyond worthless. They are intentionally undermining public health and scientific knowledge. The fact that the public doesn't notice or care is disheartening to say the least. Also, I like that guy's pinned tweet:
|
|
|
|
|
[#12]
Originally Posted By Obelix45: The CDC is beyond worthless. They are intentionally undermining public health and scientific knowledge. The fact that the public doesn't notice or care is disheartening to say the least. The CDC is returning to it's glory days of producing junk studies on gun control and similar issues, with the data carefully selected and massaged to support the predetermined conclusion. |
|
|
|
|
[#13]
Originally Posted By Obelix45: Thanks for sharing. The CDC is beyond worthless. They are intentionally undermining public health and scientific knowledge. The fact that the public doesn't notice or care is disheartening to say the least. Also, I like that guy's pinned tweet:
Originally Posted By Obelix45: Originally Posted By FlashMan-7k: Something to keep an eye out for:
Thanks for sharing. The CDC is beyond worthless. They are intentionally undermining public health and scientific knowledge. The fact that the public doesn't notice or care is disheartening to say the least. Also, I like that guy's pinned tweet:
Maybe they already know the answer because they funded the research into this bioweapon |
|
|
|
|
[#14]
Originally Posted By JPN: The CDC is returning to it's glory days of producing junk studies on gun control and similar issues, with the data carefully selected and massaged to support the predetermined conclusion. Originally Posted By JPN: Originally Posted By Obelix45: The CDC is beyond worthless. They are intentionally undermining public health and scientific knowledge. The fact that the public doesn't notice or care is disheartening to say the least. The CDC is returning to it's glory days of producing junk studies on gun control and similar issues, with the data carefully selected and massaged to support the predetermined conclusion. Middle of the worse world health crisis since 1918 and the CDC ( and congress ) is concerned about 'gun violence 'studies makes you wonder what is really going on. |
|
|
|
|
[Last Edit: FlashMan-7k]
[#15]
Originally Posted By Obelix45: Thanks for sharing. The CDC is beyond worthless. They are intentionally undermining public health and scientific knowledge. The fact that the public doesn't notice or care is disheartening to say the least. Also, I like that guy's pinned tweet:
Originally Posted By Obelix45: Originally Posted By FlashMan-7k: Something to keep an eye out for:
Thanks for sharing. The CDC is beyond worthless. They are intentionally undermining public health and scientific knowledge. The fact that the public doesn't notice or care is disheartening to say the least. Also, I like that guy's pinned tweet:
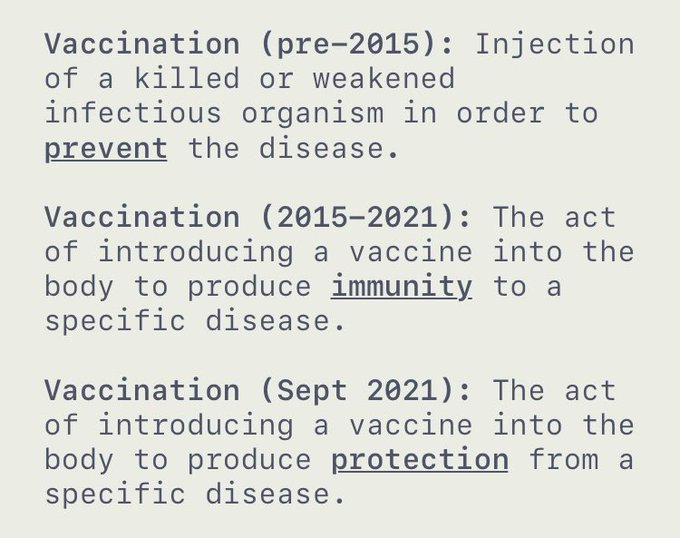
 https://technofog.substack.com/p/cdc-emails-our-definition-of-vaccine CDC Emails: Our Definition of Vaccine is "Problematic" CDC: Problematic Vaccine? No, Problematic Definition of Vaccine. Techno Fog 3 hr ago 72 32 Pic unrelated :) The CDC caused an uproar in early September 2021, after it changed its definitions of "vaccination" and "vaccine." For years, the CDC had set definitions for vaccination/vaccine that discussed immunity. This all changed on September 1, 2021. The prior CDC Definitions of Vaccine and Vaccination (August 26, 2021):
Twitter avatar for @RepThomasMassieThomas Massie @RepThomasMassie To many observers, it appeared the CDC changed the definitions because of the waning effectiveness of the COVID-19 vaccines. The effectiveness of the Pfizer vaccine falls over time, with an Israeli study reported in August 2021 as showing the vaccine being "only 16% effective against symptomatic infection for those individuals who had two doses of the shot back in January." The CDC recognizes their waning effectiveness, thus explaining their promotion of booster shots. Of course, the usual suspects defended the CDC. The Washington Post, for example, cast doubt that the CDC changed the definition because of issues with the COVID-19 vaccines. The CDC tried to downplay the change, stating "slight changes in wording over time haven't impacted the overall definition." Internal CDC E-Mails CDC emails we obtained via the Freedom of Information Act reveal CDC concerns with how the COVID-19 vaccines didn't match the CDC's own definition of "vaccine"/"vaccination". It was the CDC's Ministry of Truth hard at work in the face of legitimate public questions. In one August 2021 e-mail, a CDC employee cited to complaints that "Right-wing covid-19 deniers are using your 'vaccine' definition to argue that mRNA vaccines are not vaccines" 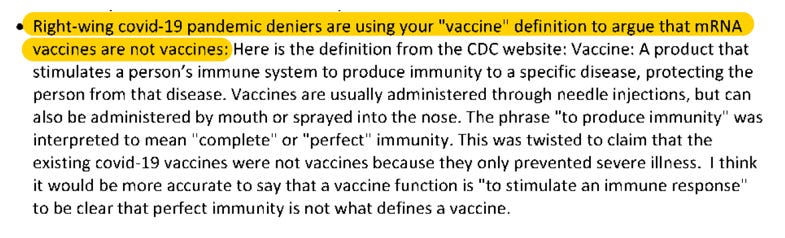 After taking some suggestions, the CDC's Lead Health Communication Specialist went up the food chain to propose changes to the definitions: "I need to update this page Immunization Basics | CDC since these definitions are outdated and being used by some to say COVID-19 vaccines are not vaccines per CDC's own definition." 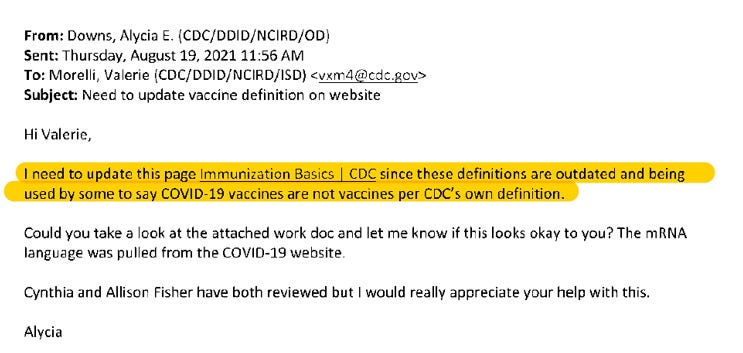 Getting no response, there was a follow-up e-mail a week later: "The definition of vaccine we have posted is problematic and people are using it to claim the COVID-19 vaccine is not a vaccine based on our own definition." The change of the "vaccination" definition was eventually approved on August 31. The next day, on September 1, they approved the change to the "vaccine" definition from discussing immunity to protection (seen below). 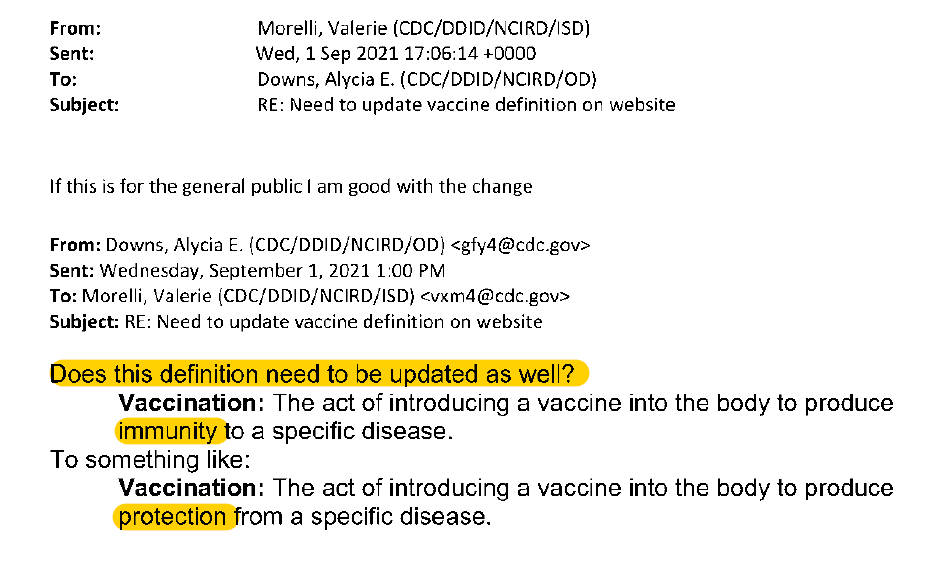 There you have it. Affirmative action for the multinational corporations. Why have them improve their vaccines when you can just change the definition of vaccine to fit their ineffective vaccines? Congrats to all the skeptics out there you raised enough concerns that the the CDC went and tried to change reality. |
|
|
|
|
[Last Edit: BlackTuono]
[#16]
We have a new paper to digest:
https://www.mdpi.com/1999-4915/13/10/2056/htm From the journal Viruses. Synopsis - in vitro experiments have confirmed that spike proteins 1) concentrate around the nucleus in a cell 2) interfere with BRCA1 and other natural DNA repair mechanisms including 3) V(D)J recombination which is is an essential part of B and T cell development and building adaptive immunity (https://en.wikipedia.org/wiki/V) This gives a putative mechanism for two anecdotal claims that have been circulating, mainly that T cells (CD4+ and CD8 in particular) get incredibly low for some people after the second and subsequent doses, and that cancer cell activity is heightened because of the lack of immune response. In this case it isn't just the response of immune cells that is being moderated but the intracellular action to repair DNA. In case you didn't know, you all have cancer inside of you, pretty much guaranteed at any given time. Cells proliferate and encounter DNA replication errors when they split, leading to cancer eventually. Our bodies employ mechanisms to repair nicked or miscopied DNA at an intracellular level constantly. Showing that T cells can be affected is one thing, but the disruption of such a fundamental biochemical repair process is alarming when you consider we are instructing cells to churn out the spike protein itself. The authors make this point in their conclusions and propose it as a putative mechanism for some of the shot-related side effects being observed. Are we going to see a lot more cancer and AIDS-like symptoms? Hopefully not in most cases, but some people are going to get unlucky and have this effect them chronically, especially if we enter a regime where regular boosters become the norm. |
|
|
|
|
[#17]
Originally Posted By HighDesert6920: Yes, and groceries. Not necessarily for the virus so much anymore - the fomite transmission has pretty much been shown to be minimal - but for the virus and everything else. A study from several years ago (long before the chinese virus) found feces on nearly 3/4 shopping carts. Look at the people in wally world next to you....they are wiping, picking, and licking all kinds of things....the fat hairy weirdo in line ahead of you is picking his nose, swiping his greasy hair back, farts and then reaches down to scratch his ass....then goes tap, tap, tap on the payment terminal....maybe sneezes in your direction...he was rummaging through all those bags of chips just before you picked out a bag. So his nasty crotch snot is smeared across the top of your chip bag....now you've got the munchies, and open the bag of chips, rubbing your hands through that guys snot, and then you grab a handful of chips and snarf them down....infected snot and all! What about those delicious apples you enjoy? Ever drive by an apple orchard during picking season? Of course, they're all illegals - but anyway, notice where the porta-potty units are - at the edge of the field...no hand washing stations to be seen....last night was chalupa night at Dos Gringos....makes Taco Bell look like quality...the guys in the field just went there last night for cheap beer and chalupas, now they have feel a power growler coming on right before picking shift. It's a mess in there! Unfortunately no hand washing stations...so just wipe hands on pants, and start picking fresh apples for the rich gringos. Now at the store, the apples are all coated with....something...something you're going to eat - because cleaning foods before eating is for pussy doomers! You're so brave! Originally Posted By HighDesert6920: Originally Posted By fl-ar-fan: Originally Posted By 79CJ7: Originally Posted By Gunner226: Unless I really take a turn for the worse, I'd put my personal experience in the "moderate cold" catagory, so far. I realize some aren't so lucky, but forcing a vaccine for this is BS. Especially a vaccine that is showing less and less efficacy - if it ever had any efficacy to begin with. This is certainly not the zombie apocalypse virus some of us thought it might turn out to be last January. 740,000 Americans might disagree with you. If they were still around. You still disinfect your mail, don't you? A study from several years ago (long before the chinese virus) found feces on nearly 3/4 shopping carts. Look at the people in wally world next to you....they are wiping, picking, and licking all kinds of things....the fat hairy weirdo in line ahead of you is picking his nose, swiping his greasy hair back, farts and then reaches down to scratch his ass....then goes tap, tap, tap on the payment terminal....maybe sneezes in your direction...he was rummaging through all those bags of chips just before you picked out a bag. So his nasty crotch snot is smeared across the top of your chip bag....now you've got the munchies, and open the bag of chips, rubbing your hands through that guys snot, and then you grab a handful of chips and snarf them down....infected snot and all! What about those delicious apples you enjoy? Ever drive by an apple orchard during picking season? Of course, they're all illegals - but anyway, notice where the porta-potty units are - at the edge of the field...no hand washing stations to be seen....last night was chalupa night at Dos Gringos....makes Taco Bell look like quality...the guys in the field just went there last night for cheap beer and chalupas, now they have feel a power growler coming on right before picking shift. It's a mess in there! Unfortunately no hand washing stations...so just wipe hands on pants, and start picking fresh apples for the rich gringos. Now at the store, the apples are all coated with....something...something you're going to eat - because cleaning foods before eating is for pussy doomers! You're so brave! I think you got a bug, because you certainly have diarrhea of the mouth. I don't eat my mail, so I don't understand your dissertation and how disinfecting mail relates to washing food off before you eat it. But, I don't understand a lot of what you doomers do either. |
|
|
|
|
[#18]
Originally Posted By BlackTuono: We have a new paper to digest: https://www.mdpi.com/1999-4915/13/10/2056/htm From the journal Viruses. Synopsis - in vitro experiments have confirmed that spike proteins 1) concentrate around the nucleus in a cell 2) interfere with BRCA1 and other natural DNA repair mechanisms including 3) V(D)J recombination which is is an essential part of B and T cell development and building adaptive immunity (https://en.wikipedia.org/wiki/V) This gives a putative mechanism for two anecdotal claims that have been circulating, mainly that T cells (CD4+ and CD8 in particular) get incredibly low for some people after the second and subsequent doses, and that cancer cell activity is heightened because of the lack of immune response. In this case it isn't just the response of immune cells that is being moderated but the intracellular action to repair DNA. In case you didn't know, you all have cancer inside of you, pretty much guaranteed at any given time. Cells proliferate and encounter DNA replication errors when they split, leading to cancer eventually. Our bodies employ mechanisms to repair nicked or miscopied DNA at an intracellular level constantly. Showing that T cells can be affected is one thing, but the disruption of such a fundamental biochemical repair process is alarming when you consider we are instructing cells to churn out the spike protein itself. The authors make this point in their conclusions and propose it as a putative mechanism for some of the shot-related side effects being observed. e Are we going to see a lot more cancer and AIDS-like symptoms? Hopefully not in most cases, but some people are going to get unlucky and have this effect them chronically, especially if we enter a regime where regular boosters become the norm.  |
|
|
|
|
[#19]
Originally Posted By BlackTuono: We have a new paper to digest: https://www.mdpi.com/1999-4915/13/10/2056/htm From the journal Viruses. Synopsis - in vitro experiments have confirmed that spike proteins 1) concentrate around the nucleus in a cell 2) interfere with BRCA1 and other natural DNA repair mechanisms including 3) V(D)J recombination which is is an essential part of B and T cell development and building adaptive immunity (https://en.wikipedia.org/wiki/V) This gives a putative mechanism for two anecdotal claims that have been circulating, mainly that T cells (CD4+ and CD8 in particular) get incredibly low for some people after the second and subsequent doses, and that cancer cell activity is heightened because of the lack of immune response. In this case it isn't just the response of immune cells that is being moderated but the intracellular action to repair DNA. In case you didn't know, you all have cancer inside of you, pretty much guaranteed at any given time. Cells proliferate and encounter DNA replication errors when they split, leading to cancer eventually. Our bodies employ mechanisms to repair nicked or miscopied DNA at an intracellular level constantly. Showing that T cells can be affected is one thing, but the disruption of such a fundamental biochemical repair process is alarming when you consider we are instructing cells to churn out the spike protein itself. The authors make this point in their conclusions and propose it as a putative mechanism for some of the shot-related side effects being observed. Are we going to see a lot more cancer and AIDS-like symptoms? Hopefully not in most cases, but some people are going to get unlucky and have this effect them chronically, especially if we enter a regime where regular boosters become the norm. The vaccine causes cancer and aids now lmao |
|
|
|
|
[#20]
... this stuff is the crud that keeps on giving.
https://elifesciences.org/articles/69314 https://elifesciences.org/download/aHR0cHM6Ly9jZG4uZWxpZmVzY2llbmNlcy5vcmcvYXJ0aWNsZXMvNjkzMTQvZWxpZmUtNjkzMTQtdjEucGRmP2Nhbm9uaWNhbFVyaT1odHRwczovL2VsaWZlc2NpZW5jZXMub3JnL2FydGljbGVzLzY5MzE0/elife-69314-v1.pdf?_hash=EmvRHSELeW1%2B6TaCi5lceBOonxLdiPrMYzpcuPgcMEE%3D Effect of SARS-CoV-2 proteins on vascular permeability Rossana Rauti, Meishar Shahoha, Yael Leichtmann-Bardoogo, Rami Nasser, Eyal Paz, Rina Tamir, Victoria Miller, Tal Babich, Kfir Shaked Department of Biomedical Engineering, Tel Aviv University, Israel; School of Neurobiology, Biochemistry and Biophysics, The George S. Wise Faculty of Life Sciences, Tel Aviv University, Israel; Sagol School of Neuroscience, Tel Aviv University, Israel; Blavatnik School of Computer Science, Tel Aviv University, Israel; Grass Center for Bioengineering, The Hebrew University of Jerusalem, Israel; The Center for Nanoscience and Nanotechnology, Tel Aviv University, Israel Research Article Oct 25, 2021 Cited 0 Views 1,400 Cite as: eLife 2021;10:e69314 doi: 10.7554/eLife.69314 Abstract Severe acute respiratory syndrome (SARS)-CoV-2 infection leads to severe disease associated with cytokine storm, vascular dysfunction, coagulation, and progressive lung damage. It affects several vital organs, seemingly through a pathological effect on endothelial cells. The SARS-CoV-2 genome encodes 29 proteins, whose contribution to the disease manifestations, and especially endothelial complications, is unknown. We cloned and expressed 26 of these proteins in human cells and characterized the endothelial response to overexpression of each, individually. Whereas most proteins induced significant changes in endothelial permeability, nsp2, nsp5_c145a (catalytic dead mutant of nsp5), and nsp7 also reduced CD31, and increased von Willebrand factor expression and IL-6, suggesting endothelial dysfunction. Using propagation-based analysis of a protein–protein interaction (PPI) network, we predicted the endothelial proteins affected by the viral proteins that potentially mediate these effects. We further applied our PPI model to identify the role of each SARS-CoV-2 protein in other tissues affected by coronavirus disease (COVID-19). While validating the PPI network model, we found that the tight junction (TJ) proteins cadherin-5, ZO-1, and β-catenin are affected by nsp2, nsp5_c145a, and nsp7 consistent with the model prediction. Overall, this work identifies the SARS-CoV-2 proteins that might be most detrimental in terms of endothelial dysfunction, thereby shedding light on vascular aspects of COVID-19. Introduction Coronavirus disease (COVID-19) caused by the 2019 novel coronavirus (2019-nCoV/SARS-CoV-2) led to a global pandemic in 2020. By late September 2021, coronavirus had infected more than 220 million people worldwide, causing over 4.5 million deaths. After the initial phase of the viral infection, ~ 30% of patients hospitalized with COVID-19 develop severe disease with progressive lung damage, known as severe acute respiratory syndrome (SARS), and a severe immune response. Interestingly, additional pathologies have been observed, such as hypoxemia and cytokine storm which, in some cases, lead to heart and kidney failure, and neurological symptoms. Recent observations suggest that these pathologies are mainly due to increased coagulation and vascular dysfunction (Lee et al., 2021; Libby and Lüscher, 2020; Siddiqi et al., 2020). It is currently believed that in addition to being a respiratory disease, COVID-19 might also be a ‘vascular disease’ (Lee et al., 2021), as it may result in a leaky vascular barrier and increased expression of von Willebrand factor (VWF) (Siddiqi et al., 2020), responsible for increased coagulation, cytokine release, and inflammation (Siddiqi et al., 2020; Teuwen et al., 2020; Aid et al., 2020; Potus et al., 2020; Wazny et al., 2020; Pum et al., 2021; Barbosa et al., 2021; Lin et al., 2020; Matarese et al., 2020; Xiao et al., 2020). Recent studies suggest that the main mechanism disrupting the endothelial barrier occurs in several stages: First, a direct effect on the endothelial cells that causes an immune response of the vascular endothelium (endotheliitis) and endothelial dysfunction. Second, lysis and death of the endothelial cells Teuwen et al., 2020; Xiao et al., 2020 followed by sequestering of human angiotensin I-converting enzyme 2 (hACE2) by viral spike proteins that activate the kallikrein–bradykinin and renin–angiotensin pathways, increasing vascular permeability (Teuwen et al., 2020; Varga et al., 2020). Last, overreaction of the immune system, during which a combination of neutrophils and immune cells producing reactive oxygen species, inflammatory cytokines (e.g., interleukin [IL]-1β, IL-6, and tumor necrosis factor), and vasoactive molecules (e.g., thrombin, histamine, thromboxane A2, and vascular endothelial growth factor), and the deposition of hyaluronic acid lead to disruption of endothelial junctions, increased vascular permeability, and leakage and coagulation (Libby and Lüscher, 2020; Teuwen et al., 2020; Varga et al., 2020). Of great interest is the effect on the brain’s vascular system. Cerebrovascular effects have been suggested to be among the long-lasting effects of COVID-19. Indeed, the susceptibility of brain endothelial cells to direct SARS-CoV-2 infection was found to increase due to increased expression of hACE2 in a blood flow-dependent manner, leading to a unique gene expression process that might contribute to the cerebrovascular effects of the virus (Pober and Sessa, 2007). While many studies point out the importance of the vascular system in COVID-19 (Kaneko et al., 2021; Jung et al., 2020b; Nägele et al., 2020), only a few Pons et al., 2020; Chioh et al., 2020; Nascimento Conde et al., 2020; Buzhdygan et al., 2020 have looked at the direct vascular response to the virus. Most of those reports stem from either clinical observations, or in vitro studies or in vivo studies in which animals/cells were transfected with the SARS-CoV-2 virus and their systemic cellular response assessed, without pinpointing the specific viral protein(s) causing the observed changes. SARS-CoV-2 is an enveloped virus with a positive-sense, single-stranded RNA genome of ∼30 kb, encoding 29 proteins (Figure 1). These proteins can be classified as: structural proteins: S (spike proteins), E (envelope proteins), M (membrane proteins), N (nucleocapsid protein and viral RNA); nonstructural proteins: nsp1–16; open reading frame accessory proteins: orf3–10 (Kim et al., 2020; Hu et al., 2021). Table 1 summarizes the known effects of specific SARS-CoV-2 proteins (Gordon et al., 2020; Peng et al., 2020b; Procko, 2020; Cornillez-Ty et al., 2009; Romano et al., 2020; Hillen et al., 2020; Chi et al., 2003). The functionality of some of these is still unknown. Moreover, a considerable knowledge gap still exists regarding molecular mechanisms, especially the protein–protein interaction (PPI) pathways (Cowen et al., 2017), leading to tissue dysfunction. Figure 1 Effect of severe acute respiratory syndrome (SARS)-CoV-2 proteins on endothelial cells. (a) Sketch representing the main organs affected by SARS-CoV-2; (b) structure and gene composition of SARS-CoV-2. Table 1 Severe acute respiratory syndrome (SARS)-CoV-2 proteins. SARS-CoV-2 proteinsGeneral impact Structural proteins S (spike)Spike protein, mediates binding to ACE2, fusion with host membrane Surface glycoprotein, needs to be processed by cellular protease TMPRSS2 (Gordon et al., 2020) M (membrane)Membrane glycoprotein, the predominant component of the envelope A major driver for virus assembly and budding (Gordon et al., 2020) E (envelope)Envelope protein, involved in virus morphogenesis and assembly Coexpression of M and E is sufficient for virus-like particle formation and release (Gordon et al., 2020) N (nucleocapsid)Nucleocapsid phosphoprotein binds to RNA genome (Gordon et al., 2020) Nonstructural proteins nsp1Leader sequence, suppresses host antiviral response Antagonizes interferon induction to suppress host antiviral response (Gordon et al., 2020) nsp2Interferes with host cell signaling, including cell cycle, cell-death pathways, and cell differentiation May serve as an adaptor for nsp3 Not essential for virus replication, but deletion of nsp2 diminishes viral growth and RNA synthesis (Gordon et al., 2020; Procko, 2020) nsp3nsp3–nsp4–nsp6 complex involved in viral replication Functions as papain-like protease (Gordon et al., 2020) nsp4nsp3–nsp4–nsp6 complex involved in viral replication (Gordon et al., 2020) The complex is predicted to nucleate and anchor viral replication complexes on double-membrane vesicles in the cytoplasm (mitochondria) nsp5Inhibits interferon I signaling processes by intervening in the NF-κB process and breaking down STAT one transcription factor Functions as 3-chymotrypsin-like protease, cleaves the viral polyprotein (Gordon et al., 2020) nsp5_c145aCatalytic dead mutant of nsp5 (Gordon et al., 2020) nsp6nsp3–nsp4–nsp6 complex involved in viral replication Limits autophagosome expansion Components of the mitochondrial complex V (the complex regenerates ATP from ADP) copurify with nsp6 (Gordon et al., 2020) nsp7Cofactor of nsp12 nsp7–nsp8 complex in part of RNA polymerase (nsp7, 8, 12 – replication complex)Affects electron transport, GPCR signaling, and membrane trafficking (Gordon et al., 2020; Peng et al., 2020b; Romano et al., 2020; Hillen et al., 2020) nsp8Cofactor of nsp12 nsp7–nsp8 complex in part of RNA polymerase. Affects the signal recognition particle and mitochondrial ribosome (Gordon et al., 2020; Peng et al., 2020b; Romano et al., 2020; Chi et al., 2003) nsp9ssRNA binding protein (can bind both DNA and RNA, but prefers ssRNA) Interacts with the replication complex (nsp7, 8, 12) (Cornillez-Ty et al., 2009) nsp10Cofactor of nsp16 and nsp14 (Romano et al., 2020) Essential for nsp16 methyltransferase activity (stimulator of nsp16) Zinc finger protein essential for replication (Gordon et al., 2020; Peng et al., 2020b) nsp11Unknown function nsp12Functions as an RNA-direct RNA polymerase, the catalytic subunitAffects the spliceosome (Gordon et al., 2020; Peng et al., 2020b; Romano et al., 2020; Hillen et al., 2020) nsp13Has helicase and 5’ triphosphatase activity Initiates the first step in viral mRNA capping nsp13,14,16 installs the cap structure onto viral mRNA in the cytoplasm instead of in the nucleus, where the host mRNA is capped (Gordon et al., 2020; Peng et al., 2020b; Romano et al., 2020; Ivanov et al., 2004) nsp14In addition to the capping function of the methyltransferase, nsp14 is also an endonuclease (3’–5’ exoribonuclease) that corrects mutations during genome replication (Gordon et al., 2020; Peng et al., 2020b; Romano et al., 2020) nsp15Endoribonuclease has uridine-specific endonuclease activity, essential for viral RNA synthesis (Gordon et al., 2020; Romano et al., 2020) nsp16May involve complexation with nsp10 and nsp14, for stabilization of homoenzyme, for capping the mRNA (Gordon et al., 2020; Peng et al., 2020b; Romano et al., 2020) Open reading frame (accessory factors) orf3aPackaging into virions Mediates trafficking of spike protein by providing ER/golgi retention signals Induces IL-6b, activates NF-κB, activates the NLRP3 inflammasome (Gordon et al., 2020) orf3bInterferon antagonist and involved in pathogenesis (Gordon et al., 2020) orf6Type I interferon antagonist, suppresses the induction of interferon, and interferon signaling pathways (Gordon et al., 2020) orf7aMay be related to viral-induced apoptosis (Gordon et al., 2020) orf7bUnknown function orf8Recombination hotspot Induces ER stress and activates NLRP3 inflammasomes Low similarity to SAR-CoV (Gordon et al., 2020) orf9bSuppresses host antiviral response Targets the mitochondrion-associated adaptor molecules MAVS and limits host cell interferon responses (Gordon et al., 2020) orf9cNo evidence that this protein is expressed during SARS-CoV-2 infection (Gordon et al., 2020) orf10No evidence that this protein is expressed during SARS-CoV-2 infection (Gordon et al., 2020) To tackle these challenges, we cultured human umbilical vein endothelial cells (HUVECs) and systematically transduced them with lentiviral particles encoding 26 out of the 29 viral proteins, separately. The three remaining genes were not included in this study purely for technical reasons. We then examined their effects on HUVEC monolayer permeability and the expression of factors involved in vascular permeability and coagulation. The results were analyzed in the context of virus–host and host–host PPI networks. By combining the insights from the experimental and computational results, we generated a model that explains how each of the 26 proteins of SARS-CoV-2, including a mutated form of nsp5, the catalytic dead mutant termed nsp5_c145a, affects the protein network regulating vascular functionality. Moreover, once the PPI model was validated with our experimental data, we applied it to more than 250 proteins that have been identified in the literature as affected by the SARS-CoV-2 proteins. This enabled us to pinpoint the more dominant SARS-CoV-2 proteins and chart their effects. Overall, this work shows how each of the SARS-CoV-2 proteins differentially affects vascular functionality; moreover, once the model was validated, we applied it to identify how SARS-CoV-2 proteins interact with proteins that have been significantly correlated with changes in cell functionality. Results SARS-CoV-2 proteins impair barrier properties affecting cell-junction proteins Increasing numbers of studies indicate a significant role for the vasculature in the physiological response to SARS-CoV-2. However, neither the exact molecular mechanism that leads to these effects nor the individual contribution of any of the SARS-CoV-2 proteins is known. Plasmids encoding SARS-CoV-2 proteins were cloned into lentivirus vectors, with eGFP-encoding vector used as a negative control. To shed light on the vascular response to the virus, HUVECs were cultured on different platforms, transduced with these lentiviral particles, and assessed for the effects of the virus proteins on different functionalities. Culturing HUVEC on Transwells or glass coverslips (Figure 2a) allowed us to identify how the specific proteins affect endothelial functionality. To ensure proper infection, the control vector included a GFP label, which enabled us to estimate infection efficiency at around 70 % (Figure 2a). Since the most basic function of the endothelium is to serve as a barrier, we sought to identify the changes in endothelium permeability in response to the SARS-CoV-2 proteins, and to pinpoint which of these proteins have the most significant effect. Barrier functions and properties were measured via trans-epithelial-endothelial electrical resistance (TEER), a standard method that identifies changes in impedance values, reflecting the integrity and permeability of the cell monolayer (Srinivasan et al., 2015). The GFP control and nine SARS-CoV-2 proteins did not show any significant change in TEER values (compared to the untreated condition), whereas 18 of the SARS-CoV-2 proteins caused significant changes in value (see plot in Figure 2b). The most dominant permeability changes were observed with nsp5_c145a, nsp13, nsp7, orf7a, and nsp2, with a 20–28% decrease in TEER values (Figure 2—figure supplement 1, and Figure 2c), in which the different SARS-CoV-2 proteins are listed and the gradual color change from red to violet represents the progressive reduction in TEER values. Figure 2—figure supplement 1 shows the comparison in TEER values before the infection and 3 and 4 days after the infection, showing that the permeability changes in the cells exposed to the viral proteins are maintained. Figure 2 with 1 supplement Effect of severe acute respiratory syndrome (SARS)-CoV-2 proteins on human umbilical vein endothelial cell (HUVEC) at day 3. (a) Bright-field and fluorescent image of infected eGFP HUVEC, scale bar: 50 µm; (b) changes in barrier functions as a result of SARS-CoV-2 proteins were assessed by trans-epithelial-endothelial … Next, we analyzed some of the proteins that exhibited the most significant (nsp2, nsp5_c145a, and nsp7) or least significant (S) changes in TEER value for changes in expression of the cell-junction proteins such as CD31 (Figure 2d and e), cadherin 1–5, occludin, and ZO 1–3 (presented later), indicating altered barrier functions. Analysis of the immunocytochemistry (ICC) (Figure 2d and e) showed, as expected, that nsp2, nsp5_c145a, and nsp7 significantly reduce the expression levels of CD31 compared to the untreated, eGFP, and S conditions, suggesting a deterioration in barrier function. Hence, these data show a differential effect of SARS-CoV-2 proteins on endothelial functionality and provide a mechanistic explanation for the reduction in endothelial integrity. Increased endothelial inflammatory response caused by SARS-CoV-2 proteins It is known that SARS-CoV-2 can cause a severe cytokine storm (Pum et al., 2021; Wang et al., 2020a) and a significant increase in coagulation-related pathologies. As we were interested in identifying the role of the vasculature in these observations, we stained and analyzed the expression level of VWF (Figure 3a and b), which is highly correlated with coagulation (Rietveld et al., 2019). Similar to the CD31 staining, we characterized only those proteins that resulted in a significant decrease in TEER values (nsp2, nsp5_c145a, and nsp7). As shown in Figure 3a and b, the control samples did not exhibit marked expression of VWF, whereas the cells transfected with nsp2, nsp5_c145a, and nsp7 showed a significant change in VWF expression. Moreover, as VWF is also associated with increased inflammation (Kawecki et al., 2017), we monitored changes in cytokine expression due to the different SARS-CoV-2 proteins (Figure 3c). We were particularly interested in IL-6, which has been identified as one of the most dominant cytokines expressed due to SARS-CoV-2 infection (Wang et al., 2020a; Akbari and Rezaie, 2020; Peruzzi et al., 2020; Liao et al., 2020b; Liao et al., 2020a). We observed that 13 out of the 26 proteins caused an increase in IL-6 secretion, 3 of which had resulted in a decrease in barrier function and increased VWF expression. Figure 3 Human umbilical vein endothelial cell (HUVEC) response to specific proteins. (a) Confocal reconstructions of HUVEC stained for von Willebrand factor (VWF) (green) and Hoechst (blue) for three conditions: control (untreated), eGFP, and nsp5_c145a, scale bar: 20 µm; (b) … Correlation between vascular permeability impairment and viral proteins We then investigated how SARS-CoV-2 causes the observed changes in HUVECs permeability. We collected sets of proteins responsible for specific functionalities of endothelial cells. We also constructed an integrated viral–host and host–host PPI network. For each viral protein and each prior functional set, we measured the network proximity between the viral protein and the human functional set using a network propagation algorithm. We scored the significance of these propagation calculations by comparing them to those obtained on random PPI networks with the same node degrees. Proteins receiving high and significant scores were most likely to interact with the specific SARS-CoV-2 protein and thus might cause the observed functional changes. When comparing the overall effects of the 26 SARS-CoV-2 proteins on endothelial TJ proteins (e.g., cadherin 1–5, occludin, and ZO 1–3), we found a correlation between the effects of the SARS-CoV-2 proteins and TEER values (Figure 4a). Moreover, some of the proteins that significantly affected the TEER parameters (Figure 2c) were also observed to be significantly proximal to the permeability-related set. These included nsp2, nsp7, and nsp13 (Figure 4a). Our algorithm identified cadherin-2, α-catenin, β-catenin, δ-catenin, and ZO 1 and 2 as the most susceptible proteins to SARS-CoV-2 infection (Figure 4b). Figure 4 Correlation between viral protein effect on permeability and proximity to permeability-related proteins in a protein–protein interaction (PPI) network. (a) Correlation of adjusted p-value versus permeability (Pearson = 0.295); (b) proximity between vascular proteins and the viral proteins. To validate our PPI network model, we performed immunostaining of some TJ proteins (β-catenin, cadherin-5, ZO-1, and occludin) of HUVEC transfected with viral proteins and to compare it to the model prediction. Similar to the CD31 staining, we characterized only those proteins that significantly decreased TEER values (nsp2, nsp5_c145a, and nsp7) compared to the eGFP and untreated condition (Figure 5). As shown in Figure 5a–c, the cells transfected with nsp2, nsp5_c145a, and nsp7 showed a significant reduction in the β-catenin, cadherin-5, and ZO-1 intensity, confirming the ability of the SARS-CoV-2 proteins to impair endothelial permeability. Figure 5 Tight-junctions impairment by severe acute respiratory syndrome (SARS)-CoV-2 proteins. Immunocytochemistry (ICC) for (a) β-catenin (green), (b) cadherin-5 (green), (c) ZO-1 (green), (d) occludin (green), and Hoechst (blue) for five specified conditions: untreated, eGFP, nsp2, … Once the model was validated, we used it to identify how the individual SARS-Cov-2 proteins affect nine other different vascular endothelial cells. As a starting point, we created a table (Table 2) (based on the literature) where we compared the expression of 12 different TJ proteins across nine different types of endothelial cells. We then applied the network-based model to identify which endothelial cells are more susceptible to the different SARS-Cov-2 proteins. As can be seen in Figure 6, there are significant differences in the response of various viral proteins on different types of vascular endothelial cells. For example,, the viral proteins nsp13, nsp11, orf6, and S seem to have a significant effect on the different types of vascular endothelial cells, according to the network score detected. However, the proteins m, E, n, nsp12, and nsp8 are the less interactive with the vascular cells. Table 2 Comparison of tight junction (TJ) proteins expression among different types of vascular endothelial cells. Endothelial cells typeTJ proteins Cadherin-2Cadherin-3Cadherin-4Cadherin-5δ-1-Cateninβ-Cateninα-CateninOccludinClaudin-5ZO-1ZO-2ZO-3 Human pulmonary artery endothelial cells (HPAECs) (Nakato et al., 2019; Chi et al., 2003; Ivanov et al., 2004; Ferreri et al., 2008; DiStefano et al., 2014; Zebda et al., 2013; Yuan et al., 2012; Wang et al., 2011)+−−++++++++− Human umbilical vein endothelial cells (HUVECs) (Nakato et al., 2019; Chi et al., 2003; Ferreri et al., 2008; Wu et al., 2008; Dean et al., 2009; Polus et al., 2006; DeBusk et al., 2010; Wessells et al., 2009)++++++++++++ Human umbilical artery endothelial cells (HUAECs) (Nakato et al., 2019; Chi et al., 2003; Davis et al., 2003; Ikuno et al., 2017; Kevil et al., 1998; Kluger et al., 2013)−+−+++−+++++ Human great saphenous vein endothelial cells (HGSVECs) (Nakato et al., 2019; Chi et al., 2003; Latif et al., 2006; Murakami et al., 2008)−−−++−++++++ Human common carotid artery endothelial cells (HCCaECs) (Nakato et al., 2019; Chi et al., 2003)+−+−−+−+++++ Human aortic endothelial cells (HAoECs) (Nakato et al., 2019; Chi et al., 2003; Wu et al., 2017; Sandig et al., 1999; DeMaio et al., 2006)−−−−−+++++++ Human coronary artery endothelial cells (HCAECs) (Nakato et al., 2019; Chi et al., 2003; Wessells et al., 2009; Wu et al., 2004; Pinto et al., 2018)−−++++++++++ Human endocardial cells (HENDCs) (Nakato et al., 2019; Chi et al., 2003; Vestweber et al., 2009; Bao et al., 2017)+−−+−+++++−− Human renal artery endothelial cells (HRAECs) (Nakato et al., 2019; Chi et al., 2003; Maciel et al., 2018)−−++−+−+++−− Figure 6 Correlation between viral proteins and different types of vascular endothelial cells. Correlation of adjusted p-value between vascular proteins identified in vascular endothelial cells and the viral proteins. As our network propagation model is highly correlated with our experimental results, we applied it to other physiological systems that are known to be affected by SARS-CoV-2. We created a list of all proteins that are known to be affected by the SARS-CoV-2 proteins according to the literature (Supplementary file 1A, white columns). The table was composed of both proteins identified experimentally via western blot, proteomics, and immunohistochemistry (marked in blue) and those identified clinically as being highly correlated with loss of specific functionality in specific tissues (marked in red). We then applied the network-based model to identify which proteins in Supplementary file 1A are most susceptible to the different SARS-CoV-2 proteins. As can be seen in Figure 7—figure supplements 2–7, Supplementary file 1A and B, specific SARS-CoV-2 proteins were identified as affecting specific proteins in specific tissues. As expected, most of the SARS-CoV-2 proteins affected more than one protein, the most salient being nsp11, nsp4, and nsp7 (Figure 7b), each of which was predicted to affect more than 40 different proteins. An additional parameter that should be considered is the protein’s ‘distance’ from the viral proteins. This value represents the number of hops in the PPI network from a given protein to the viral proteins, where a value of 1 represents a direct viral–host connection. We hypothesized that the closer the distance between the viral proteins and the given protein, the more significant the viral effect. Supplementary file 1A (gray columns) and Figure 7c present the calculated distances. Most of the identified proteins in Supplementary file 1A were classified with a distance of 1 or 2 from the virus, suggesting more severe putative effects. A very clear example, are the T cells, macrophages, lung epithelial and cardiomyocytes which show that the most significant effect was by the viral proteins which present a close connection with the relative cell proteins reported. This suggest a potential effect on the related functional or metabolic pathway (Supplementary file 1A). Figure 7 with 7 supplements Protein identification using protein–protein interaction (PPI). (a) PPI results for the severe acute respiratory syndrome (SARS)-CoV-2 proteins that have a significant effect on the proteins presented in SI Table 1 for each system; (b) number of proteins … Discussion Due to the impact of SARS-CoV-2, many studies have looked at the physiological responses to the virus (Lee et al., 2021; Libby and Lüscher, 2020; Siddiqi et al., 2020; Teuwen et al., 2020; Chioh et al., 2020). In this work, we sought to identify how specific SARS-CoV-2 proteins affect the vasculature by assessing the effect of individual SARS-CoV-2 proteins on endothelial cells (HUVEC). This approach has significant advantages: it enables pinpointing and isolating how each of the SARS-CoV-2 proteins independently affects the endothelial response, and directly measuring endothelial functionality. The HUVEC model, derived from the umbilical cord, is physiologically representative of the human vascular endothelium, allowing the study of the physiological and pathological conditions as well as the effects of novel drugs on human endothelium (Bouïs et al., 2001; Medina-Leyte et al., 2020). Among technical advantages, cultured HUVECs are a simple in vitro vascular endothelial model, particularly suitable for studying endothelial properties and dynamics as well as the putative role of adhesion molecules, the synthesis of extracellular proteins and blood vessel maturation (Vailhé et al., 2001). The current study showed that almost 70 % (18 out of 26) of the SARS-CoV-2 proteins affect endothelial barrier integrity; however, the most significant proteins were nsp2, nsp5_c145a, and nsp7, which also induced upregulated expression of the coagulation factor VWF and cytokine release. These critical facts can shed light on the multiple pathologies observed in SARS-CoV-2 infection, including cytokine storm, increased coagulation and related diseases (e.g., heart attack and stroke) (Lee et al., 2021; Aid et al., 2020), increased cardiovascular disease, and increased neurological symptoms. The results presented here showed an effect of in vitro cultured endothelial cells, which may lead to vasculature leakiness, consequently causing exotoxicity (i.e., the penetration of toxic reagents from the blood into the brain). While there are many parameters associated with functional changes, the use of advanced tools, including network-based analysis, enabled us to elucidate the specific proteins and the specific interactions that are predicted to cause these changes. The PPI network enabled us to predict that the changes observed in barrier function are possibly due to interactions between host proteins such as cadherin 2, α-catenin, β-catenin, δ-catenin, and ZO 1 and 2, and at least with the viral proteins nsp2, nsp5_c145a, and nsp7. Moreover, we validated our PPI model performing further immunostaining analysis demonstrating not only the ability of the viral proteins to strongly impair TJ expression, but also to confirm the data predicted by our model in which some TJ proteins can be more affected than others. PPI analysis revealed a highly correlated effect of nsp7 and nsp13 on β-catenin in endothelial cells (Figure 4b; Jung et al., 2020a; Lengfeld et al., 2017). Interestingly, neither nsp2 nor nsp5_c145a affected a high number of proteins (Figure 7b), whereas nsp7 did, as identified by the network. Analyzing the repertoire of SARS-CoV-2 proteins, we see almost no effect of the structural proteins; rather, mostly nonstructural and open reading frame proteins affected HUVEC functionality, manifested as decreased barrier function and increased cytokine secretion (Figures 2 and 3). While the nonstructural proteins are mainly responsible for replicating viral RNA, the open reading frame proteins are related to counteraction with the host immune system; some of these are localized to the mitochondria and have been shown to alter the mitochondrial antiviral signaling pathway (Miller et al., 2021). We found that the proteins most affecting barrier function (decreased TEER and decreased CD31, β-catenin, cadherin-5, and ZO-1 expression) and cytokine response (IL-6 secretion and VWF expression) were nsp2, nsp5_c145a, and nsp7 (Figure 2; Figure 3; Figure 6); nsp7 forms a replication complex with nsp8 and nsp12 that is essential for viral replication and transcription (Cowen et al., 2017; Peng et al., 2020a). Peng et al., 2020b suggested that in the core polymerase complex nsp7–nsp8–nsp12, nsp12 is the catalytic subunit, and nsp7 and nsp8 function as cofactors. They further suggested that the mechanism of activation mainly involves the cofactors rather than the catalytic subunit (Peng et al., 2020b). This might explain why we saw mainly an effect of the cofactor proteins on endothelial cells and almost no effect of the catalytic subunit. Network interactions Díaz, 2020 have shown that nsp7 has the most interactions with the host, suggesting a potential target for the treatment of COVID-19. Moreover, no mutations were found in nsp7 compared to nsp2 or nsp5_c145a (Kaushal et al., 2020), suggesting a conserved protein with a vital function in virus survival. The nsp13 protein has both helicase activity and 5’ triphosphatase activity, which play an important role in mRNA capping. We saw a significant effect of nsp13 on barrier function, but hardly any effect on cytokine secretion. Chen et al., 2020, suggested functional complexation between nsp8 and nsp12, the RdRp (RNA-dependent RNA polymerase) replication complex, and nsp13. Given the fact that we observed a substantial effect of nsp7 – one of the proteins of the replication complex – and an effect of nsp13 on HUVEC barrier function, complexation of nsp13 with the replication complex might indicate an important role for this complex in the impaired functionality of the HUVECs, and therefore in the propagation of the disease, and the known vascular damage seen in COVID-19 patients. As suggested by our model, nsp13 seems to have a strong effect also on other types of vascular endothelial cells (Figure 6) as well as on all cell types (Figure 7a), positioning nsp13 as one of the main targets for disease treatment. It is important to note that the comparison between the different endothelial cell types revealed exciting differences in the TJ protein expression, which correlate to the different properties of the different cell types (Nakato et al., 2019). One of the major differences was that some endothelial cell lines do not have cadherin at all (e.g., HAoEC), or very limited amount of cadherin (e.g., HPAEC, HUAEC, HGSVEC). Our model suggests that some endothelial types (e.g., HUVEC, HUAEC, HGSVEC, HCAEC) are more susceptible to the SARS-Cov-2 virus. It, therefore, suggests that the treatment of one type of endothelial cell might be different from another type but offers the PPI model as a tool for initial prediction. Overall, the combination of identifying the differences in the TJ protein expression between the different endothelial cells and the use of the PPI model enabled us to pinpoint the differences in susceptibility to the disease and to identify which specific proteins have the most significant effect. Many studies have looked at the SARS-CoV-2 interaction with nonpulmonary/nonvascular tissues (e.g., neurons, hepatocytes, immune components such as lymphocytes, macrophages, etc.) (Lee et al., 2021), as pathological studies identified a viral effect on these tissues, despite their very limited amount, or lack of ACE2 receptors. To better understand how SARS-CoV-2 interacts with and affects other tissues, we consolidated all of the proteins currently known to be affected by the virus into Supplementary file 1A. It is interesting to note that the most dominant SARS-CoV-2 proteins are nsp4, nsp11, and nsp7. Davies et al., 2020, identified the interaction of nsp2 with nsp4, both involved in endoplasmic reticulum (ER) calcium signaling and mitochondrial biogenesis. This suggests a new functional role in the host ER and mitochondrial organelle contact process and calcium homeostasis. By now it is clear that vasculature plays a significant role in the physiological response to the virus. However, it is still unclear how the virus affects the vasculature, and if it can be found in the blood. This is a critical question, as it has significant consequences on the extent of the virus’s ability to affect the vasculature. Current studies demonstrate that the pulmonary vasculature is significantly affected and is one of the dominant triggers for the pathologies mentioned above. However, involvement with the rest of the vasculature is still unclear, as is whether the virus can be found in an active form in the blood circulation (Peng et al., 2020a; Chang et al., 2020; Orologas-Stavrou et al., 2020; Andersson et al., 2020; Escribano et al., 2020; Wang et al., 2020b). Some studies suggest that even if there are traces of SARS-CoV-2 in the blood, it is not in an active form and cannot cause disease or a systemic response (Andersson et al., 2020). On the other hand, some studies suggest that SARS-CoV-2 can be found in the blood, and can induce the disease and cause both cellular and systemic dysfunction (Peng et al., 2020a; Chang et al., 2020; Escribano et al., 2020). While this question is beyond the scope of this work, it is important to note that if future studies do identify the active form of SARS-CoV-2 in human blood, then the implications of our findings will apply to this systemic response as well (Ahmed et al., 2020; Park et al., 2020). As already noted, the pathology is probably a combination of multiple conditions and pathways activated by the different proteins. However, our findings might open new avenues for future therapeutics. Moreover, most of the proteins that were identified as affected by SARS-CoV-2 had a distance factor of at most three to the human and viral proteins. This coincides with the current dogma, whereby proteins that have a shorter distance between them are more likely to be affected. While beneficial, our approach has two major limitations: (a) our inability to identify the effect of multiple proteins and (b) our neglect of the effect of the coronavirus structure and binding on the cellular response. The former point can be overcome by expressing combinations of different SARS-CoV-2 proteins. However, since the SARS-CoV-2 expresses 29 proteins, there are about ~9 × 1030 possible protein combinations. Therefore, we decided to focus on individual proteins and allow further studies to pursue any combinations of interest. Regarding the latter limitation, we did not include the coronavirus structure (including the ACE2 receptors) in this study, because many studies have already demonstrated the cellular response to this structure (Chioh et al., 2020; Yang et al., 2020; Procko, 2020), and how tissues that do not have significant ACE2 expression (neurons, immune components such as B and T lymphocytes, and macrophages) are affected by the virus remains an open question. Conclusions Accumulating clinical evidence suggests that COVID-19 is a disease with vascular aspects. However, only a few studies have identified the specific role of each of the SARS-CoV-2 proteins in the cellular response leading to vascular dysfunctions. In this work, we characterized the endothelial response to each of 26 SARS-CoV-2 proteins and identified those that have the most significant effect on the barrier function. In addition, we used PPI network-based analysis to predict which of the endothelial proteins is most affected by the virus and to identify the specific role of each of the SARS-CoV-2 proteins in the observed changes in systemic protein expression. Overall, this work identified which of the SARS-CoV-2 proteins are most dominant in their effect on the physiological response to the virus. We believe that the data presented in this work will give us better insight into the mechanism by which the vasculature and the system respond to the virus, and will enable us to expedite drug development for the virus by targeting the identified dominant proteins. Materials and methods Generation of lentiviral SARS-CoV-2 plasmids Request a detailed protocol Plasmids encoding the SARS-CoV-2 open reading frames proteins and eGFP control were a kind gift of Nevan Krogan (Addgene plasmid #141367–141395). Plasmids were acquired as bacterial LB–agar stabs and used per the provider’s instructions. Briefly, each stab was first seeded in LB agar (Bacto Agar; BD Biosciences, San Jose, CA) in 10 cm plates. Then, single colonies were inoculated into flasks containing LB (BD Difco LB Broth, Lennox) and 100 µg/ml penicillin (Biological Industries, Beit HaEmek, Israel). Transfection-grade plasmid DNA was isolated from each flask using the ZymoPURE II Plasmid Maxiprep Kit (Zymo Research, Irvine, CA) according to the manufacturer’s instructions. Lentivirus preparation Request a detailed protocol HEK293T cells (ATCC, Manassas, VA) were seeded in 10 cm cell culture plates at a density of 4 × 106 cells/plate. The cells were maintained in 293T medium composed of DMEM high glucose (4.5 g/l; Merck, Rahway, NJ) supplemented with 10 % fetal bovine serum (FBS; Biological Industries), 1× NEAA (Biological Industries), and 2 mM L-alanine–L-glutamine (Biological Industries, Israel). Lentiviral stocks, pseudo-typed with VSV-G, were produced in HEK293T cells as previously described (Kutner et al., 2009). Briefly, each of the pLVX plasmids containing the SARS-CoV-2 genes or EGFP for control were cotransfected with third-generation lentivirus helper plasmids at equimolar ratio; 48 hr later, the lentivirus-containing medium was collected and supernatant was clarified by centrifugation (500 g, 5 min) and filtration (0.45 µm, Millex-HV, Merck Millipore, Burlington, MA). All virus stocks were aliquoted and stored at –80 °C until thawed for subsequent use. Endothelial cell culture Request a detailed protocol HUVECs (C-12200, PromoCell GmbH, Heidelberg, Germany, tested negative for mycoplasma contamination) were used to test each viral protein’s impact on vascular properties. After thawing, the HUVECs were expanded in low-serum endothelial cell growth medium (PromoCell) at 37°C with 5% CO2 in a humidifying incubator, and used at passage p4–p6. Cells were grown to 80–90% confluence before being transferred to transparent polyethylene terephthalate Transwell supports (0.4 µm pore size, Greiner Bio-One, Austria) or a glass-bottom well plate (Cellvis, Mountain View, CA). Before seeding, the uncoated substrates were treated with Entactin-Collagen IV-Laminin (ECL) Cell Attachment Matrix (Merck) diluted in DMEM (10 µg/cm2) for 1 hr in the incubator. Then, the HUVECs were harvested using a DetachKit (PromoCell), were seeded inside the culture platforms at a density of 250,000 cells/cm2, and grown for 3 days. Then viral infection with the different plasmids was performed and its impact on cell behavior was tested 3 days later. TEER measurement Request a detailed protocol The barrier properties of the endothelial monolayer were evaluated by TEER measurements, 3 and 4 days after viral infection. TEER was measured with the Millicell ERS-2 Voltohmmeter (Merck Millipore). TEER values (Ω cm2) were calculated and compared to those obtained in a Transwell insert without cells, considered as a blank, in three different individual experiments, with two inserts used for each viral protein. Immunofluorescence Request a detailed protocol HUVEC plated on glass-bottom plates were rinsed in phosphate buffered saline (PBS) and fixed in 4 % paraformaldehyde (Sigma-Aldrich, Rehovot, Israel) for 20 min at RT, 5 days after viral infection. ICC was carried out after permeabilization with 0.1 % Triton X-100 (Sigma-Aldrich, Rehovot, Israel) in PBS for 10 min at RT and blocking for 30 min with 5 % FBS in PBS. The following primary antibodies were applied overnight in PBS at 4°C: rabbit anti-VWF (Abcam, Cambridge, UK), rabbit anti-CD31 (Abcam) against platelet endothelial cell adhesion molecule 1 (PECAM1), rabbit anti-β-catenin (Cell Signaling Technology, Danvers, MA), rabbit anti-cadherin-5 (Cell Signaling Technology, Danvers, MA), rabbit anti ZO-1 (Cell Signaling Technology, Danvers, MA), rabbit anti-occludin (Cell Signaling Technology, Danvers, MA). Cells were then washed three times in PBS and stained with the secondary antibody, anti-rabbit Alexa Fluor 488 (Invitrogen, Carlsbad, CA), for 1 hr at RT. After four washes with PBS, cells were incubated with Hoechst in PBS for 10 min at RT to stain the nuclei. After two washes with PBS, imaging was carried out using an inverted confocal microscope (Olympus FV3000-IX83) with suitable filter cubes and equipped with 20× (0.8 NA), 40× (0.95 NA), and 60× (1.42 NA) objectives. Image reconstruction and analysis were done using open-source ImageJ software (Schindelin et al., 2012). Network analysis Request a detailed protocol We scored the effect of each viral protein on selected human proteins using network propagation (Cowen et al., 2017). Specifically, a viral protein was represented by the set of its human interactors (Hu et al., 2021); each of these received a prior score, equal to 1 /n, where n is the size of the interactor set; these scores were propagated in a network of PPI (Almozlino et al., 2017). To assess the statistical significance of the obtained scores, we compared them to those computed on 1000 randomized networks that preserve node degrees. The PPI score was then compared versus the other random networks (this is empirical p-value). p-Values were adjusted for multiple testing using Benjamini–Hochberg FDR approach. For display purposes, the plotted p-value is the negative log of the p-value, which means numbers are non-negative and the higher is the more significant. Quantitative ELISA for IL-6 Request a detailed protocol ELISA was performed on conditioned medium of infected HUVEC 3 days postinfection, according to the manufacturer’s recommendations (PeproTech Rehovot, Israel). Statistical analysis Request a detailed protocol The results are presented as mean ± SD, unless otherwise indicated. Statistically significant differences among multiple groups were evaluated by F-statistic with two-way ANOVA, followed by the Holm–Sidak test for multiple comparisons (GraphPad Prism 8.4.3). The difference between the two data sets was assessed and p < 0.05 was considered statistically significant. Data availability All data generated or analysed during this study are included in the manuscript and supporting files. The custom scripts available in GitHub: https://github.com/raminass/covid_networks, (copy archived at https://archive.softwareheritage.org/swh:1:rev:b239ae7e0e72b722beb6d694436068541ea28dbb). References Ahmed H Sayed A Munir M Elberry MH Sayed IM Kamal MA Negida A Ebada MA Bahbah EI (2020) A Clinical Review of COVID-19; Pathogenesis, Diagnosis, and Management Current Pharmaceutical Design 1:509. https://doi.org/10.2174/1381612826666201222162509 PubMed Google Scholar Aid M Busman-Sahay K Vidal SJ Maliga Z Bondoc S Starke C Terry M Jacobson CA Wrijil L Ducat S Brook OR Miller AD Porto M Pellegrini KL Pino M Hoang TN Chandrashekar A Patel S Stephenson K Bosinger SE Andersen H Lewis MG Hecht JL Sorger PK Martinot AJ Estes JD Barouch DH (2020) Vascular Disease and Thrombosis in SARS-CoV-2-Infected Rhesus Macaques Cell 183:1354–1366. https://doi.org/10.1016/j.cell.2020.10.005 PubMed Google Scholar Akbari A Rezaie J (2020) Potential therapeutic application of mesenchymal stem cell-derived exosomes in SARS-CoV-2 pneumonia Stem Cell Research & Therapy 11:356. https://doi.org/10.1186/s13287-020-01866-6 PubMed Google Scholar Almozlino Y Atias N Silverbush D Sharan R (2017) ANAT 2.0: reconstructing functional protein subnetworks BMC Bioinformatics 18:495. https://doi.org/10.1186/s12859-017-1932-1 PubMed Google Scholar Andersson MI Arancibia-Carcamo CV Auckland K Baillie JK Barnes E Beneke T Bibi S Brooks T Carroll M Crook D Dingle K Dold C Downs LO Dunn L Eyre DW Gilbert Jaramillo J Harvala H Hoosdally S Ijaz S James T James W Jeffery K Justice A Klenerman P Knight JC Knight M Liu X Lumley SF Matthews PC McNaughton AL Mentzer AJ Mongkolsapaya J Oakley S Oliveira MS Peto T Ploeg RJ Ratcliff J Robbins MJ Roberts DJ Rudkin J Russell RA Screaton G Semple MG Skelly D Simmonds P Stoesser N Turtle L Wareing S Zambon M (2020) SARS-CoV-2 RNA detected in blood products from patients with COVID-19 is not associated with infectious virus Wellcome Open Research 5:181. https://doi.org/10.12688/wellcomeopenres.16002.2 PubMed Google Scholar Bao X Bhute VJ Han T Qian T Lian X Palecek SP (2017) Human pluripotent stem cell-derived epicardial progenitors can differentiate to endocardial-like endothelial cells Bioengineering & Translational Medicine 2:191–201. https://doi.org/10.1002/btm2.10062 PubMed Google Scholar Barbosa LC Gonçalves TL de Araujo LP de Rosario L Ferrer VP (2021) Endothelial cells and SARS-CoV-2: An intimate relationship Vascular Pharmacology 137:106829. https://doi.org/10.1016/j.vph.2021.106829 PubMed Google Scholar Bouïs D Hospers GA Meijer C Molema G Mulder NH (2001) Endothelium in vitro: a review of human vascular endothelial cell lines for blood vessel-related research Angiogenesis 4:91–102. https://doi.org/10.1023/a:1012259529167 PubMed Google Scholar Buzhdygan TP DeOre BJ Baldwin-Leclair A Bullock TA McGary HM Khan JA Razmpour R Hale JF Galie PA Potula R Andrews AM Ramirez SH (2020) The SARS-CoV-2 spike protein alters barrier function in 2D static and 3D microfluidic in-vitro models of the human blood-brain barrier Neurobiology of Disease 146:105131. https://doi.org/10.1016/j.nbd.2020.105131 PubMed Google Scholar Chang L Yan Y Wang L (2020) Coronavirus Disease 2019: Coronaviruses and Blood Safety Transfusion Medicine Reviews 34:75–80. https://doi.org/10.1016/j.tmrv.2020.02.003 PubMed Google Scholar Chen J Malone B Llewellyn E Grasso M Shelton PMM Olinares PDB Maruthi K Eng ET Vatandaslar H Chait BT Kapoor TM Darst SA Campbell EA (2020) Structural Basis for Helicase-Polymerase Coupling in the SARS-CoV-2 Replication-Transcription Complex Cell 182:1560–1573. https://doi.org/10.1016/j.cell.2020.07.033 PubMed Google Scholar Chi JT Chang HY Haraldsen G Jahnsen FL Troyanskaya OG Chang DS Wang Z Rockson SG van de Rijn M Botstein D Brown PO (2003) Endothelial cell diversity revealed by global expression profiling PNAS 100:10623–10628. https://doi.org/10.1073/pnas.1434429100 PubMed Google Scholar Preprint Chioh FWJ Fong SW Young BE (2020) Convalescent COVID-19 Patients Are Susceptible to Endothelial Dysfunction Due to Persistent Immune Activation medRxiv. https://doi.org/10.1101/2020.11.16.20232835v1 Google Scholar Cornillez-Ty CT Liao L Yates JR Kuhn P Buchmeier MJ (2009) Severe acute respiratory syndrome coronavirus nonstructural protein 2 interacts with a host protein complex involved in mitochondrial biogenesis and intracellular signaling Journal of Virology 83:10314–10318. https://doi.org/10.1128/JVI.00842-09 PubMed Google Scholar Cowen L Ideker T Raphael BJ Sharan R (2017) Network propagation: a universal amplifier of genetic associations Nature Reviews. Genetics 18:551–562. https://doi.org/10.1038/nrg.2017.38 PubMed Google Scholar Davies JP Almasy KM McDonald EF Plate L (2020) Comparative Multiplexed Interactomics of SARS-CoV-2 and Homologous Coronavirus Nonstructural Proteins Identifies Unique and Shared Host-Cell Dependencies ACS Infectious Diseases 6:3174–3189. https://doi.org/10.1021/acsinfecdis.0c00500 PubMed Google Scholar Davis MA Ireton RC Reynolds AB (2003) A core function for p120-catenin in cadherin turnover The Journal of Cell Biology 163:525–534. https://doi.org/10.1083/jcb.200307111 PubMed Google Scholar Dean WL Lee MJ Cummins TD Schultz DJ Powell DW (2009) Proteomic and functional characterisation of platelet microparticle size classes Thrombosis and Haemostasis 102:711–718. https://doi.org/10.1160/TH09-04-243 PubMed Google Scholar DeBusk LM Boelte K Min Y Lin PC (2010) Heterozygous deficiency of delta-catenin impairs pathological angiogenesis The Journal of Experimental Medicine 207:77–84. https://doi.org/10.1084/jem.20091097 PubMed Google Scholar DeMaio L Rouhanizadeh M Reddy S Sevanian A Hwang J Hsiai TK (2006) Oxidized phospholipids mediate occludin expression and phosphorylation in vascular endothelial cells American Journal of Physiology. Heart and Circulatory Physiology 290:H674–H683. https://doi.org/10.1152/ajpheart.00554.2005 PubMed Google Scholar Díaz J (2020) SARS-CoV-2 Molecular Network Structure Frontiers in Physiology 11:870. https://doi.org/10.3389/fphys.2020.00870 PubMed Google Scholar DiStefano PV Kuebel JM Sarelius IH Glading AJ (2014) KRIT1 protein depletion modifies endothelial cell behavior via increased vascular endothelial growth factor (VEGF) signaling The Journal of Biological Chemistry 289:33054–33065. https://doi.org/10.1074/jbc.M114.582304 PubMed Google Scholar Escribano P Álvarez-Uría A Alonso R Catalán P Alcalá L Muñoz P Guinea J (2020) Detection of SARS-CoV-2 antibodies is insufficient for the diagnosis of active or cured COVID-19 Scientific Reports 10:19893. https://doi.org/10.1038/s41598-020-76914-5 PubMed Google Scholar Ferreri DM Minnear FL Yin T Kowalczyk AP Vincent PA (2008) N-cadherin levels in endothelial cells are regulated by monolayer maturity and p120 availability Cell Communication & Adhesion 15:333–349. https://doi.org/10.1080/15419060802440377 PubMed Google Scholar Gordon DE Jang GM Bouhaddou M Xu J Obernier K White KM O’Meara MJ Rezelj VV Guo JZ Swaney DL Tummino TA Hüttenhain R Kaake RM Richards AL Tutuncuoglu B Foussard H Batra J Haas K Modak M Kim M Haas P Polacco BJ Braberg H Fabius JM Eckhardt M Soucheray M Bennett MJ Cakir M McGregor MJ Li Q Meyer B Roesch F Vallet T Mac Kain A Miorin L Moreno E Naing ZZC Zhou Y Peng S Shi Y Zhang Z Shen W Kirby IT Melnyk JE Chorba JS Lou K Dai SA Barrio-Hernandez I Memon D Hernandez-Armenta C Lyu J Mathy CJP Perica T Pilla KB Ganesan SJ Saltzberg DJ Rakesh R Liu X Rosenthal SB Calviello L Venkataramanan S Liboy-Lugo J Lin Y Huang XP Liu Y Wankowicz SA Bohn M Safari M Ugur FS Koh C Savar NS Tran QD Shengjuler D Fletcher SJ O’Neal MC Cai Y Chang JCJ Broadhurst DJ Klippsten S Sharp PP Wenzell NA Kuzuoglu-Ozturk D Wang HY Trenker R Young JM Cavero DA Hiatt J Roth TL Rathore U Subramanian A Noack J Hubert M Stroud RM Frankel AD Rosenberg OS Verba KA Agard DA Ott M Emerman M Jura N von Zastrow M Verdin E Ashworth A Schwartz O d’Enfert C Mukherjee S Jacobson M Malik HS Fujimori DG Ideker T Craik CS Floor SN Fraser JS Gross JD Sali A Roth BL Ruggero D Taunton J Kortemme T Beltrao P Vignuzzi M García-Sastre A Shokat KM Shoichet BK Krogan NJ (2020) A SARS-CoV-2 protein interaction map reveals targets for drug repurposing Nature 583:459–468. https://doi.org/10.1038/s41586-020-2286-9 PubMed Google Scholar Hillen HS Kokic G Farnung L Dienemann C Tegunov D Cramer P (2020) Structure of replicating SARS-CoV-2 polymerase Nature 584:154–156. https://doi.org/10.1038/s41586-020-2368-8 PubMed Google Scholar Hu B Guo H Zhou P Shi ZL (2021) Characteristics of SARS-CoV-2 and COVID-19 Nature Reviews. Microbiology 19:141–154. https://doi.org/10.1038/s41579-020-00459-7 PubMed Google Scholar Ikuno T Masumoto H Yamamizu K Yoshioka M Minakata K Ikeda T Sakata R Yamashita JK Rajasingh J (2017) Efficient and robust differentiation of endothelial cells from human induced pluripotent stem cells via lineage control with VEGF and cyclic AMP PLOS ONE 12:e0173271. https://doi.org/10.1371/journal.pone.0173271 PubMed Google Scholar Ivanov KA Thiel V Dobbe JC van der Meer Y Snijder EJ Ziebuhr J (2004) Multiple enzymatic activities associated with severe acute respiratory syndrome coronavirus helicase Journal of Virology 78:5619–5632. https://doi.org/10.1128/JVI.78.11.5619-5632.2004 PubMed Google Scholar Jung Y Park GS Moon JH Ku K Beak SH Lee CS Kim S Park EC Park D Lee JH Byeon CW Lee JJ Maeng JS Kim SJ Kim SI Kim BT Lee MJ Kim HG (2020a) Comparative Analysis of Primer-Probe Sets for RT-qPCR of COVID-19 Causative Virus (SARS-CoV-2 ACS Infectious Diseases 6:2513–2523. https://doi.org/10.1021/acsinfecdis.0c00464 PubMed Google Scholar Jung F Krüger-Genge A Franke RP Hufert F Küpper JH (2020b) COVID-19 and the endothelium Clinical Hemorheology and Microcirculation 75:7–11. https://doi.org/10.3233/CH-209007 Google Scholar Kaneko N Satta S Komuro Y Muthukrishnan SD Kakarla V Guo L An J Elahi F Kornblum HI Liebeskind DS Hsiai T Hinman JD (2021) Flow-Mediated Susceptibility and Molecular Response of Cerebral Endothelia to SARS-CoV-2 Infection Stroke 52:260–270. https://doi.org/10.1161/STROKEAHA.120.032764 PubMed Google Scholar Kaushal N Gupta Y Goyal M Khaiboullina SF Baranwal M Verma SC (2020) Mutational Frequencies of SARS-CoV-2 Genome during the Beginning Months of the Outbreak in USA Pathogens 9:E565. https://doi.org/10.3390/pathogens9070565 PubMed Google Scholar Kawecki C Lenting PJ Denis CV (2017) von Willebrand factor and inflammation Journal of Thrombosis and Haemostasis 15:1285–1294. https://doi.org/10.1111/jth.13696 PubMed Google Scholar Kevil CG Okayama N Trocha SD Kalogeris TJ Coe LL Specian RD Davis CP Alexander JS (1998) Expression of zonula occludens and adherens junctional proteins in human venous and arterial endothelial cells: role of occludin in endothelial solute barriers Microcirculation 5:197–210. PubMed Google Scholar Kim D Lee JY Yang JS Kim JW Kim VN Chang H (2020) The Architecture of SARS-CoV-2 Transcriptome Cell 181:914–921. https://doi.org/10.1016/j.cell.2020.04.011 PubMed Google Scholar Kluger MS Clark PR Tellides G Gerke V Pober JS (2013) Claudin-5 controls intercellular barriers of human dermal microvascular but not human umbilical vein endothelial cells Arteriosclerosis, Thrombosis, and Vascular Biology 33:489–500. https://doi.org/10.1161/ATVBAHA.112.300893 PubMed Google Scholar Kutner RH Zhang XY Reiser J (2009) Production, concentration and titration of pseudotyped HIV-1-based lentiviral vectors Nature Protocols 4:495–505. https://doi.org/10.1038/nprot.2009.22 PubMed Google Scholar Latif N Sarathchandra P Taylor PM Antoniw J Brand N Yacoub MH (2006) Characterization of molecules mediating cell-cell communication in human cardiac valve interstitial cells Cell Biochemistry and Biophysics 45:255–264. https://doi.org/10.1385/CBB:45:3:255 PubMed Google Scholar Lee MH Perl DP Nair G Li W Maric D Murray H Dodd SJ Koretsky AP Watts JA Cheung V Masliah E Horkayne-Szakaly I Jones R Stram MN Moncur J Hefti M Folkerth RD Nath A (2021) Microvascular Injury in the Brains of Patients with Covid-19 The New England Journal of Medicine 384:481–483. https://doi.org/10.1056/NEJMc2033369 PubMed Google Scholar Lengfeld JE Lutz SE Smith JR Diaconu C Scott C Kofman SB Choi C Walsh CM Raine CS Agalliu I Agalliu D (2017) Endothelial Wnt/β-catenin signaling reduces immune cell infiltration in multiple sclerosis PNAS 114:E1168–E1177. https://doi.org/10.1073/pnas.1609905114 PubMed Google Scholar Liao Y Li X Mou T Zhou X Li D Wang L Zhang Y Dong X Zheng H Guo L Liang Y Jiang G Fan S Xu X Xie Z Chen H Liu L Li Q (2020a) Distinct infection process of SARS-CoV-2 in human bronchial epithelial cell lines Journal of Medical Virology 92:2830–2838. https://doi.org/10.1002/jmv.26200 PubMed Google Scholar Liao M Liu Y Yuan J Wen Y Xu G Zhao J Cheng L Li J Wang X Wang F Liu L Amit I Zhang S Zhang Z (2020b) Single-cell landscape of bronchoalveolar immune cells in patients with COVID-19 Nature Medicine 26:842–844. https://doi.org/10.1038/s41591-020-0901-9 PubMed Google Scholar Libby P Lüscher T (2020) COVID-19 is, in the end, an endothelial disease European Heart Journal 41:3038–3044. https://doi.org/10.1093/eurheartj/ehaa623 PubMed Google Scholar Lin T Luo W Li Z Zhang L Zheng X Mai L Yang W Guan G Su Z Liu P Li Z Xie Y (2020) Rhamnocitrin extracted from Nervilia fordii inhibited vascular endothelial activation via miR-185/STIM-1/SOCE/NFATc3 Phytomedicine : International Journal of Phytotherapy and Phytopharmacology 79:153350. https://doi.org/10.1016/j.phymed.2020.153350 PubMed Google Scholar Maciel RAP Cunha RS Busato V Franco CRC Gregório PC Dolenga CJR Nakao LS Massy ZA Boullier A Pecoits-Filho R Stinghen AEM (2018) Uremia Impacts VE-Cadherin and ZO-1 Expression in Human Endothelial Cell-to-Cell Junctions Toxins 10:E404. https://doi.org/10.3390/toxins10100404 PubMed Google Scholar Matarese A Gambardella J Sardu C Santulli G (2020) miR-98 Regulates TMPRSS2 Expression in Human Endothelial Cells: Key Implications for COVID-19 Biomedicines 8:462. https://doi.org/10.3390/biomedicines8110462 PubMed Google Scholar Medina-Leyte DJ Domínguez-Pérez M Mercado I Villarreal-Molina MT Jacobo-Albavera L (2020) Use of Human Umbilical Vein Endothelial Cells (HUVEC) as a Model to Study Cardiovascular Disease: A Review Applied Sciences 10:938. https://doi.org/10.3390/app10030938 Google Scholar Miller B Silverstein A Flores M Cao K Kumagai H Mehta HH Yen K Kim SJ Cohen P (2021) Host mitochondrial transcriptome response to SARS-CoV-2 in multiple cell models and clinical samples Scientific Reports 11:3. https://doi.org/10.1038/s41598-020-79552-z Google Scholar Murakami M Nguyen LT Zhuang ZW Zhang ZW Moodie KL Carmeliet P Stan RV Simons M (2008) The FGF system has a key role in regulating vascular integrity The Journal of Clinical Investigation 118:3355–3366. https://doi.org/10.1172/JCI35298 PubMed Google Scholar Nägele MP Haubner B Tanner FC Ruschitzka F Flammer AJ (2020) Endothelial dysfunction in COVID-19: Current findings and therapeutic implications Atherosclerosis 314:58–62. https://doi.org/10.1016/j.atherosclerosis.2020.10.014 PubMed Google Scholar Nakato R Wada Y Nakaki R Nagae G Katou Y Tsutsumi S Nakajima N Fukuhara H Iguchi A Kohro T Kanki Y Saito Y Kobayashi M Izumi-Taguchi A Osato N Tatsuno K Kamio A Hayashi-Takanaka Y Wada H Ohta S Aikawa M Nakajima H Nakamura M McGee RC Heppner KW Kawakatsu T Genno M Yanase H Kume H Senbonmatsu T Homma Y Nishimura S Mitsuyama T Aburatani H Kimura H Shirahige K (2019) Comprehensive epigenome characterization reveals diverse transcriptional regulation across human vascular endothelial cells Epigenetics & Chromatin 12:e0319-0. https://doi.org/10.1186/s13072-019-0319-0 Google Scholar Nascimento Conde J Schutt WR Gorbunova EE Mackow ER (2020) Recombinant ACE2 Expression Is Required for SARS-CoV-2 To Infect Primary Human Endothelial Cells and Induce Inflammatory and Procoagulative Responses MBio 11:e03185-20. https://doi.org/10.1128/mBio.03185-20 PubMed Google Scholar Orologas-Stavrou N Politou M Rousakis P Kostopoulos IV Ntanasis-Stathopoulos I Jahaj E Tsiligkeridou E Gavriatopoulou M Kastritis E Kotanidou A Dimopoulos MA Tsitsilonis OE Terpos E (2020) Peripheral Blood Immune Profiling of Convalescent Plasma Donors Reveals Alterations in Specific Immune Subpopulations Even at 2 Months Post SARS-CoV-2 Infection Viruses 13:E26. https://doi.org/10.3390/v13010026 PubMed Google Scholar Park J Kim H Kim SY Kim Y Lee JS Dan K Seong MW Han D (2020) -depth blood proteome profiling analysis revealed distinct functional characteristics of plasma proteins between severe and non-severe COVID-19 patients Scientific Reports 10:22418. https://doi.org/10.1038/s41598-020-80120-8 PubMed Google Scholar Peng L Liu J Xu W Luo Q Chen D Lei Z Huang Z Li X Deng K Lin B Gao Z (2020a) SARS-CoV-2 can be detected in urine, blood, anal swabs, and oropharyngeal swabs specimens Journal of Medical Virology 92:1676–1680. https://doi.org/10.1002/jmv.25936 PubMed Google Scholar Peng Q Peng R Yuan B Zhao J Wang M Wang X Wang Q Sun Y Fan Z Qi J Gao GF Shi Y (2020b) Structural and Biochemical Characterization of the nsp12-nsp7-nsp8 Core Polymerase Complex from SARS-CoV-2 Cell Reports 31:107774. https://doi.org/10.1016/j.celrep.2020.107774 PubMed Google Scholar Peruzzi B Bencini S Capone M Mazzoni A Maggi L Salvati L Vanni A Orazzini C Nozzoli C Morettini A Poggesi L Pieralli F Peris A Bartoloni A Vannucchi AM Liotta F Caporale R Cosmi L Annunziato F (2020) Quantitative and qualitative alterations of circulating myeloid cells and plasmacytoid DC in SARS-CoV-2 infection Immunology 161:345–353. https://doi.org/10.1111/imm.13254 PubMed Google Scholar Pinto MT Ferreira Melo FU Malta TM Rodrigues ES Plaça JR Silva WA Panepucci RA Covas DT de Oliveira Rodrigues C Kashima S (2018) Endothelial cells from different anatomical origin have distinct responses during SNAIL/TGF-β2-mediated endothelial-mesenchymal transition American Journal of Translational Research 10:4065–4081. PubMed Google Scholar Pober JS Sessa WC (2007) Evolving functions of endothelial cells in inflammation Nature Reviews. Immunology 7:803–815. https://doi.org/10.1038/nri2171 PubMed Google Scholar Polus A Kiec-Wilk B Hartwich J Balwierz A Stachura J Dyduch G Laidler P Zagajewski J Langman T Schmitz G Goralczyk R Wertz K Riss G Keijer J Dembinska-Kiec A (2006) The chemotactic activity of beta-carotene in endothelial cell progenitors and human umbilical vein endothelial cells: A microarray analysis Experimental and Clinical Cardiology 11:117–122. PubMed Google Scholar Pons S Fodil S Azoulay E Zafrani L (2020) The vascular endothelium: the cornerstone of organ dysfunction in severe SARS-CoV-2 infection Critical Care 24:353. https://doi.org/10.1186/s13054-020-03062-7 PubMed Google Scholar Potus F Mai V Lebret M Malenfant S Breton-Gagnon E Lajoie AC Boucherat O Bonnet S Provencher S (2020) Novel insights on the pulmonary vascular consequences of COVID-19 American Journal of Physiology. Lung Cellular and Molecular Physiology 319:L277–L288. https://doi.org/10.1152/ajplung.00195.2020 PubMed Google Scholar Preprint Procko E (2020) The Sequence of Human ACE2 Is Suboptimal for Binding the S Spike Protein of SARS Coronavirus 2 bioRxiv. https://doi.org/10.1101/2020.03.16.994236 Google Scholar Pum A Ennemoser M Adage T Kungl AJ (2021) Cytokines and Chemokines in SARS-CoV-2 Infections-Therapeutic Strategies Targeting Cytokine Storm Biomolecules 11:91. https://doi.org/10.3390/biom11010091 PubMed Google Scholar Rietveld IM Lijfering WM le Cessie S Bos MHA Rosendaal FR Reitsma PH Cannegieter SC (2019) High levels of coagulation factors and venous thrombosis risk: strongest association for factor VIII and von Willebrand factor Journal of Thrombosis and Haemostasis 17:99–109. https://doi.org/10.1111/jth.14343 PubMed Google Scholar Romano M Ruggiero A Squeglia F Maga G Berisio R (2020) A Structural View of SARS-CoV-2 RNA Replication Machinery: RNA Synthesis, Proofreading and Final Capping Cells 9:1267. https://doi.org/10.3390/cells9051267 PubMed Google Scholar Sandig M Korvemaker ML Ionescu CV Negrou E Rogers KA (1999) Transendothelial migration of monocytes in rat aorta: distribution of F-actin, alpha-catnin, LFA-1, and PECAM-1 Biotechnic & Histochemistry 74:276–293. https://doi.org/10.3109/10520299909034666 PubMed Google Scholar Schindelin J Arganda-Carreras I Frise E Kaynig V Longair M Pietzsch T Preibisch S Rueden C Saalfeld S Schmid B Tinevez J-Y White DJ Hartenstein V Eliceiri K Tomancak P Cardona A (2012) Fiji: an open-source platform for biological-image analysis Nature Methods 9:676–682. https://doi.org/10.1038/nmeth.2019 PubMed Google Scholar Siddiqi HK Libby P Ridker PM (2020) COVID-19 and vascular disease EBioMedicine 58:102966. https://doi.org/10.1016/j.ebiom.2020.102966 PubMed Google Scholar Srinivasan B Kolli AR Esch MB Abaci HE Shuler ML Hickman JJ (2015) TEER measurement techniques for in vitro barrier model systems Journal of Laboratory Automation 20:107–126. https://doi.org/10.1177/2211068214561025 PubMed Google Scholar Teuwen LA Geldhof V Pasut A Carmeliet P (2020) COVID-19: the vasculature unleashed Nature Reviews. Immunology 20:389–391. https://doi.org/10.1038/s41577-020-0343-0 PubMed Google Scholar Vailhé B Vittet D Feige JJ (2001) vitro models of vasculogenesis and angiogenesis Laboratory Investigation; a Journal of Technical Methods and Pathology 81:439–452. https://doi.org/10.1038/labinvest.3780252 PubMed Google Scholar Varga Z Flammer AJ Steiger P Haberecker M Andermatt R Zinkernagel AS Mehra MR Schuepbach RA Ruschitzka F Moch H (2020) Endothelial cell infection and endotheliitis in COVID-19 Lancet 395:1417–1418. https://doi.org/10.1016/S0140-6736(20)30937-5 PubMed Google Scholar Vestweber D Winderlich M Cagna G Nottebaum AF (2009) Cell adhesion dynamics at endothelial junctions: VE-cadherin as a major player Trends in Cell Biology 19:8–15. https://doi.org/10.1016/j.tcb.2008.10.001 PubMed Google Scholar Wang L Chiang ET Simmons JT Garcia JGN Dudek SM (2011) FTY720-induced human pulmonary endothelial barrier enhancement is mediated by c-Abl The European Respiratory Journal 38:78–88. https://doi.org/10.1183/09031936.00047810 PubMed Google Scholar Wang J Jiang M Chen X Montaner LJ (2020a) Cytokine storm and leukocyte changes in mild versus severe SARS-CoV-2 infection: Review of 3939 COVID-19 patients in China and emerging pathogenesis and therapy concepts Journal of Leukocyte Biology 108:17–41. https://doi.org/10.1002/JLB.3COVR0520-272R PubMed Google Scholar Wang W Xu Y Gao R Lu R Han K Wu G Tan W (2020b) Detection of SARS-CoV-2 in Different Types of Clinical Specimens JAMA 323:1843–1844. https://doi.org/10.1001/jama.2020.3786 PubMed Google Scholar Wazny V Siau A Wu KX Cheung C (2020) Vascular underpinning of COVID-19 Open Biology 10:200208. https://doi.org/10.1098/rsob.200208 PubMed Google Scholar Wessells H Sullivan CJ Tsubota Y Engel KL Kim B Olson NE Thorner D Chitaley K (2009) Transcriptional profiling of human cavernosal endothelial cells reveals distinctive cell adhesion phenotype and role for claudin 11 in vascular barrier function Physiological Genomics 39:100–108. https://doi.org/10.1152/physiolgenomics.90354.2008 PubMed Google Scholar Wu H Yao Q Lumsden A Chen C (2004) Characterization of two populations of human coronary artery endothelial cells(1 The Journal of Surgical Research 118:38–44. https://doi.org/10.1016/j.jss.2004.01.009 PubMed Google Scholar Wu JC Yan HC Chen WT Chen WH Wang CJ Chi YC Kao WY (2008) JNK signaling pathway is required for bFGF-mediated surface cadherin downregulation on HUVEC Experimental Cell Research 314:421–429. https://doi.org/10.1016/j.yexcr.2007.10.002 PubMed Google Scholar Wu M Zhang J-D Tang R-N Crowley SD Liu H Lv L-L Ma K-L Liu B-C (2017) Elevated PTH induces endothelial-to-chondrogenic transition in aortic endothelial cells American Journal of Physiology. Renal Physiology 312:F436–F444. https://doi.org/10.1152/ajprenal.00210.2016 PubMed Google Scholar Preprint Xiao J Zhang B Su Z Liu Y Shelite TR Chang Q Wang P Bukreyev A Soong L Jin Y Ksiazek T Gaitas A Rossi SL Zhou J Laposata M Saito TB Gong B (2020) EPAC Regulates von Willebrand Factor Secretion from Endothelial Cells in a PI3K/ENOS-Dependent Manner during Inflammation bioRxiv. https://doi.org/10.1101/2020.09.04.282806 Google Scholar Yang J Petitjean SJL Koehler M Zhang Q Dumitru AC Chen W Derclaye S Vincent SP Soumillion P Alsteens D (2020) Molecular interaction and inhibition of SARS-CoV-2 binding to the ACE2 receptor Nature Communications 11:4541. https://doi.org/10.1038/s41467-020-18319-6 PubMed Google Scholar Yuan L Le Bras A Sacharidou A Itagaki K Zhan Y Kondo M Carman CV Davis GE Aird WC Oettgen P (2012) ETS-related gene (ERG) controls endothelial cell permeability via transcriptional regulation of the claudin 5 (CLDN5) gene The Journal of Biological Chemistry 287:6582–6591. https://doi.org/10.1074/jbc.M111.300236 PubMed Google Scholar Zebda N Tian Y Tian X Gawlak G Higginbotham K Reynolds AB Birukova AA Birukov KG (2013) teraction of p190RhoGAP with C-terminal domain of p120-catenin modulates endothelial cytoskeleton and permeability The Journal of Biological Chemistry 288:18290–18299. https://doi.org/10.1074/jbc.M112.432757 PubMed Google Scholar Decision letter Arduino A Mangoni Reviewing Editor; Flinders Medical Centre, Australia Matthias Barton Senior Editor; University of Zurich, Switzerland Francesco Pasqualini Reviewer Gad Vatine Reviewer; Ben Gurion University In the interests of transparency, eLife publishes the most substantive revision requests and the accompanying author responses. Acceptance summary: In their manuscript, Rauti, Shahoha et al., sought to identify the effect of SARS-CoV2 proteins on endothelial functions. They systematically transduced HUVECs cultured on a transwell with various SARS-CoV2 proteins from three classes including non-structural and accessory proteins. They have assessed the effect of separate overexpression of each of 26 proteins, and tested their effect on 26 of the 29 proteins in the SARS-CoV2 genome. The authors found that overexpression of some proteins had stronger effect on the barrier functions on HUVECs compared to other proteins. Using a PPI network analysis, they predicted endothelial proteins that may be affected by the viral protein, which may potentially mediate this effect. The findings add to the understanding how SARS-CoV2 may negatively affect endothelial cell homeostasis, which may contribute to vascular and thrombotic complications associated with a severe course of the disease in patients diagnosed with COVID-19. Decision letter after peer review: Thank you for submitting your article "Effect of SARS-CoV-2 proteins on vascular permeability" for consideration by eLife. Your article has been reviewed by 2 peer reviewers, and the evaluation has been overseen by a Reviewing Editor and Matthias Barton as the Senior Editor. The following individuals involved in review of your submission have agreed to reveal their identity: Francesco Pasqualini (Reviewer #1); Gad Vatine (Reviewer #2). The reviewers have discussed their reviews with one another, and the Reviewing Editor has drafted this to help you prepare a revised submission. Essential revisions: 1) The authors provide putative virus-host protein-protein interaction networks that could be very valuable for future translational efforts. However, it would be best to validate at least one of those on the HUVECS/TEER assay. Would it be possible to rescue endothelial dysfunction acting (pharmacologically or genetically) on any of the identified host proteins downstream of the viral protein? 2) The authors provide virus-host protein interaction networks for endothelial cells of various organs. This, again, could be a very valuable target identification exercise for future pharmacological work but it would need to be validated. Can the rescue experiment discussed above be replicated using the TEER assay, organ-specific endothelial cells, and pharmacological or genetic means to normalize the expression of host proteins downstream of the viral protein in the organ-specific PPI network? 3) More validation data will help but it might be worth revising the discussion as well, especially as the new validation data may make parts of the current Discussion redundant. 4) Page 4, line 98 – "Permeability was measured via trans-epithelial-endothelial 99 electrical resistance (TEER), a standard method that identifies changes in impedance values". TEER is a method for assessing barrier functions, and it is related to permeability, but permeability should be measured by fluorescent paracellular assays. These should be separated. 5) While significant, the changes in TEER are very small. The authors should specify in the figure legend, which statistical tests have been applied, and should specify that they have accounted for multiple comparison tests. Also, changes in TEER over time should be showed. 6) In order to avoid conclusions that may be linked to direct regulation on CD31, changes in protein expression should be made on additional proteins that are related to tight junctions such as ZO1. 7) Overall, all experiments were performed on a single source of in vitro human endothelial cells. The authors should discuss possibilities for additional endothelial cell models that could potentially be used for future studies, and discuss the advantages and disadvantages of HUVECs. 8) The authors develop a mathematic model to identify interactions of the SARS-CoV2 proteins with tissue targets. While this represents a novel an important approach, authors should show a validation of the model to prove its validity. If this cannot be applied in the HUVECs system, the authors should explain its limitations and at least discuss what possible models could be used to validate it in the future. 9) Since the authors identify WNT signaling as a key pathway, the authors cold consider manipulating the WNT pathway in HUVECs cells as a possible treatment for rescuing this effect.Reviewer #1: The hypothesis of the authors is that non-spike SARS-CoV-2 proteins are responsible for the increased vascular permeability observed in COVID-19 patients during the primary infection and, possibly, long after it is resolved. To identify which protein(s) might be responsible, they used lentiviruses to express 26/29 SARS-CoV-2 proteins in human endothelial cells (HUVECS) using trans-epithelial-endothelial electrical resistance (TEER), a standard assessment of vascular permeability. Among the viral proteins that directly increased vascular permeability, the authors identified a subset (nsp2,29 nsp5_c145a (catalytic dead mutant of nsp5) and nsp7) capable of inducing broader endothelial dysfunction (downregulated CD31 and upregulated VWF and IL-6). Finally, they used protein-protein interaction analysis to semi-quantitatively speculate how these viral proteins may lead to endothelial dysfunction and increased vascular permeability in various human organs. Strengths The use of a library of LV to test each individual SARS-CoV-2 protein is interesting. While hard to use combinatorially, being able to isolate the influence of each protein will be important in understanding the secondary effect of COVID-19 infections (e.g., long COVID). The combination of imaging and TEER to screen how each viral protein changes endothelial structure, function, or both. The use of bio-informatics to relate the raw findings from the cellular assay with broader translational implications, namely through which pathways may viral protein end up affecting vascular permeability and endothelial dysfunction. Weaknesses I feel like the paper is missing two key additional validations. First, the authors provide putative virus-host protein-protein interaction networks that could be very valuable for future translational efforts. However, it would be best to validate at least one of those on the HUVECS/TEER assay. Would it be possible to rescue endothelial dysfunction acting (pharmacologically or genetically) on any of the identified host proteins downstream of the viral protein? Second, the authors provide virus-host protein interaction networks for endothelial cells of various organs. This, again, could be a very valuable target identification exercise for future pharmacological work but it would need to be validated. Can the rescue experiment discussed above be replicated using the TEER assay, organ-specific endothelial cells, and pharmacological or genetic means to normalize the expression of host proteins downstream of the viral protein in the organ-specific PPI network?Reviewer #2: In their manuscript, Rauti, Shahoha et al., sought to identify the effect of SARS-CoV2 proteins on endothelial functions. They systematically transduced HUVECs cultured on a transwell with various SARS-CoV2 proteins from three classes including non-structural and accessory proteins. They have assessed the effect of separate overexpression of each of 26 proteins, and tested their effect on 26 of the 29 proteins in the SARS-CoV2 genome. The authors found that overexpression of some proteins had stronger effect on the barrier functions on HUVECs compared to other proteins. Using a PPI network analysis, they predicted endothelial proteins that may be affected by the viral protein, which may potentially mediate this effect. The novelty of the study is in directly testing the response of endothelial cells to the virus. Previous reports focused on the phenotype in patients, or using animal models without specifying the exact proteins involved in the dysfunction. Gaining knowledge on the molecular mechanisms, especially the protein-protein interaction pathways that lead to tissue dysfunction, may help understanding the pandemic a potentially help develop treatments. https://doi.org/10.7554/eLife.69314.sa1 Author response Essential revisions: 1) The authors provide putative virus-host protein-protein interaction networks that could be very valuable for future translational efforts. However, it would be best to validate at least one of those on the HUVECS/TEER assay. Would it be possible to rescue endothelial dysfunction acting (pharmacologically or genetically) on any of the identified host proteins downstream of the viral protein? We would like to thank the referee for his suggestion. We agree that it is important to show the validity of the model before using it on other proteins. Following the referee’s suggestion, we have performed a series of experiments to validate the model (new Figure 5). Our new data present high correlation between the PPI prediction and the experimental data. 2) The authors provide virus-host protein interaction networks for endothelial cells of various organs. This, again, could be a very valuable target identification exercise for future pharmacological work but it would need to be validated. Can the rescue experiment discussed above be replicated using the TEER assay, organ-specific endothelial cells, and pharmacological or genetic means to normalize the expression of host proteins downstream of the viral protein in the organ-specific PPI network? Following the referee’s suggestion to examine different organ-specific endothelial cells, we have made a unique comparison of the expression level of the different endothelial proteins in 9 different vascular endothelial cell types (see new Table 2). Although we assumed that most proteins will be detected in these lines, we were surprised to learn that in some cell lines, like the HAoEC, all cadherin proteins (Cadherin 2-5) do not express while in others Catenin d is not expressed while in other most ZO proteins are missing. We were surprised to learn that such a comparison was never published, making this publication also unique in that way. After we validated the PPI network, we used it to examine how the specific SARS-Cov-2 proteins affect the organ-specific endothelial cells (for 9 organ-specific vascular endothelial cells). Our results presented in new Figure 6 predict that not only the HUVEC permeability properties are impaired by the SARSCov-2 proteins, but other vascular endothelial cells are strongly affected as well. Interestingly, we see that different endothelial cells response differently to SARS-Cov-2, mainly due to the different expression of the tight junctions proteins. 3) More validation data will help but it might be worth revising the discussion as well, especially as the new validation data may make parts of the current Discussion redundant. The discussion was revised according to the new validation. 4) Page 4, line 98 – "Permeability was measured via trans-epithelial-endothelial 99 electrical resistance (TEER), a standard method that identifies changes in impedance values". TEER is a method for assessing barrier functions, and it is related to permeability, but permeability should be measured by fluorescent paracellular assays. These should be separated. We thank the author for this comment. The text was revised to better clarify this point. 5) While significant, the changes in TEER are very small. The authors should specify in the figure legend, which statistical tests have been applied, and should specify that they have accounted for multiple comparison tests. Also, changes in TEER over time should be showed. In this work we used ANOVA-multiple comparison test to account for the multiple comparison among different groups. This was described in the method section and per the reviewer request, it was also added to the figure legend. The TEER dynamic is highly dependent on the cell density, age, and condition. Per the reviewer request, we added the TEER values of the cells in multiple time points (before the infection, 3 and 4 days after the infection (new Figure S1)). 6) In order to avoid conclusions that may be linked to direct regulation on CD31, changes in protein expression should be made on additional proteins that are related to tight junctions such as ZO1. We would like to thank the referee for this comment. We have performed additional set of experiments examining also the effect on ZO1 (and other 3 proteins, B-Catenin, Cadherine 5 and Occludin). The new data, now in new Figure 5, show that the viral proteins that showed a significant decrease in the TEER values as well as in the CD31 intensity, significant affect the expression of these other tight-junctions proteins. 7) Overall, all experiments were performed on a single source of in vitro human endothelial cells. The authors should discuss possibilities for additional endothelial cell models that could potentially be used for future studies, and discuss the advantages and disadvantages of HUVECs. As we discussed in “point 2”, we created a table which compares 9 organ-specific endothelial cells. We added the results as Table 2 and new Figure 6. We also revised the text accordingly. 8) The authors develop a mathematic model to identify interactions of the SARS-CoV2 proteins with tissue targets. While this represents a novel an important approach, authors should show a validation of the model to prove its validity. If this cannot be applied in the HUVECs system, the authors should explain its limitations and at least discuss what possible models could be used to validate it in the future. As we discussed in “point 2”, we created a table which compares 9 organ-specific endothelial cells. We added the results as Table 2 and new Figure 6. We also revised the text accordingly. 9) Since the authors identify WNT signaling as a key pathway, the authors cold consider manipulating the WNT pathway in HUVECs cells as a possible treatment for rescuing this effect. WNT was suggested as a relevant pathway due to its known contribution to BBB impairment in multiple sclerosis and other pathologies (Jung, Y., et al. ACS Infect. Dis. (2020); Lengfeld, J. E.,et al. Proc Natl Acad Sci (2017)). In addition, the ßcatenin is part of the WNT signaling, and we showed the validation of its effect by the SARS-Cov-2, i.e. decrease in expression caused by the virus infection. But since it is not the main claim of the paper, (the contribution of the WNT to the BBB impairment due to the SARS-Cov-2) we removed this point from the discussion. Manipulation of the WNT signaling pathway is beyond the scope of this paper. https://doi.org/10.7554/eLife.69314.sa2 Article and author information Author details Rossana Rauti Department of Biomedical Engineering, Tel Aviv University, Tel Aviv, Israel Contribution Conceptualization, Formal analysis, Methodology, Project administration, Writing – original draft Contributed equally with Meishar Shahoha and Yael Leichtmann-Bardoogo Competing interests No competing interests declared ORCID icon 0000-0001-8569-0810 Meishar Shahoha School of Neurobiology, Biochemistry and Biophysics, The George S. Wise Faculty of Life Sciences, Tel Aviv University, Tel Aviv, Israel Sagol School of Neuroscience, Tel Aviv University, Tel Aviv, Israel Contribution Conceptualization, Data curation, Investigation, Methodology, Visualization Contributed equally with Rossana Rauti and Yael Leichtmann-Bardoogo Competing interests No competing interests declared ORCID icon 0000-0001-5947-484X Yael Leichtmann-Bardoogo Department of Biomedical Engineering, Tel Aviv University, Tel Aviv, Israel Contribution Conceptualization, Data curation, Investigation, Methodology, Visualization, Writing – original draft Contributed equally with Rossana Rauti and Meishar Shahoha Competing interests No competing interests declared Rami Nasser Blavatnik School of Computer Science, Tel Aviv University, Tel Aviv, Israel Contribution Formal analysis, Software Competing interests No competing interests declared Eyal Paz School of Neurobiology, Biochemistry and Biophysics, The George S. Wise Faculty of Life Sciences, Tel Aviv University, Tel Aviv, Israel Sagol School of Neuroscience, Tel Aviv University, Tel Aviv, Israel Contribution Methodology, Writing - review and editing Competing interests No competing interests declared Rina Tamir Department of Biomedical Engineering, Tel Aviv University, Tel Aviv, Israel Contribution Formal analysis, Investigation Competing interests No competing interests declared Victoria Miller Department of Biomedical Engineering, Tel Aviv University, Tel Aviv, Israel Contribution Formal analysis, Investigation Competing interests No competing interests declared Tal Babich Department of Biomedical Engineering, Tel Aviv University, Tel Aviv, Israel School of Neurobiology, Biochemistry and Biophysics, The George S. Wise Faculty of Life Sciences, Tel Aviv University, Tel Aviv, Israel Contribution Formal analysis, Investigation Competing interests No competing interests declared Kfir Shaked Department of Biomedical Engineering, Tel Aviv University, Tel Aviv, Israel School of Neurobiology, Biochemistry and Biophysics, The George S. Wise Faculty of Life Sciences, Tel Aviv University, Tel Aviv, Israel Contribution Formal analysis, Investigation Competing interests No competing interests declared Avner Ehrlich Grass Center for Bioengineering, The Hebrew University of Jerusalem, Jerusalem, Israel Contribution Methodology, Resources Competing interests No competing interests declared Konstantinos Ioannidis Grass Center for Bioengineering, The Hebrew University of Jerusalem, Jerusalem, Israel Contribution Methodology, Resources Competing interests No competing interests declared Yaakov Nahmias Grass Center for Bioengineering, The Hebrew University of Jerusalem, Jerusalem, Israel Contribution Methodology, Resources Competing interests No competing interests declared Roded Sharan Blavatnik School of Computer Science, Tel Aviv University, Tel Aviv, Israel Contribution Formal analysis, Software Competing interests No competing interests declared Uri Ashery School of Neurobiology, Biochemistry and Biophysics, The George S. Wise Faculty of Life Sciences, Tel Aviv University, Tel Aviv, Israel Sagol School of Neuroscience, Tel Aviv University, Tel Aviv, Israel The Center for Nanoscience and Nanotechnology, Tel Aviv University, Tel Aviv, Israel Contribution Funding acquisition, Investigation, Supervision, Writing – original draft Competing interests No competing interests declared ORCID icon 0000-0001-6338-7888 Ben Meir Maoz Department of Biomedical Engineering, Tel Aviv University, Tel Aviv, Israel Sagol School of Neuroscience, Tel Aviv University, Tel Aviv, Israel The Center for Nanoscience and Nanotechnology, Tel Aviv University, Tel Aviv, Israel Contribution Conceptualization, Funding acquisition, Project administration, Supervision, Visualization, Writing – original draft For correspondence [email protected] Competing interests No competing interests declared ORCID icon 0000-0002-3823-7682 Funding Israel Science Foundation (2248/19) Rossana Rauti Yael Leichtmann-Bardoogo Rina Tamir Victoria Miller Tal Babich Kfir Shaked Ben Meir Maoz Azrieli Foundation Rossana Rauti Yael Leichtmann-Bardoogo Ben Meir Maoz Horizon 2020 (SweetBrain 851765) Rossana Rauti Yael Leichtmann-Bardoogo Ben Meir Maoz Aufzien Family Center for the Prevention and Treatment of Parkinson's Disease Rossana Rauti Meishar Shahoha Yael Leichtmann-Bardoogo Eyal Paz Rina Tamir Victoria Miller Tal Babich Kfir Shaked Uri Ashery Ben Meir Maoz Deutsche Forschungsgemeinschaft (207/10-1) Rami Nasser Avner Ehrlich Konstantinos Ioannidis Yaakov Nahmias Roded Sharan Teva Pharmaceutical Industries Yael Leichtmann-Bardoogo Ben Meir Maoz Zimin Yael Leichtmann-Bardoogo Ben Meir Maoz Ministry of Science and Technology, Israel (3-17351) Rossana Rauti Yael Leichtmann-Bardoogo Ben Meir Maoz TCCP Uri Ashery Ben Meir Maoz Israel Science Foundation (953/16) Rina Tamir Victoria Miller Tal Babich Kfir Shaked Ben Meir Maoz The funders had no role in study design, data collection and interpretation, or the decision to submit the work for publication. Acknowledgements BMM was supported by the Azrieli Foundation, Israel Science Foundation (ISF grant: 2248/19), ERC SweetBrain 851765, TEVA, The Aufzien Family Center for the Prevention and Treatment of Parkinson’s Disease at Tel Aviv University, Zimin, Israel Ministry of Science and Technology (Grant No. 3–17351), and TCCP. UA was supported by the Israel Science Foundation (ISF grant 953/16), TEVA, The Aufzien Family Center for the Prevention and Treatment of Parkinson’s Disease at Tel Aviv University, the German Research Foundation (DFG) (NA: 207/10–1) and the Taube/Koret Global Collaboration in Neurodegenerative Diseases. RS was supported by the Israel Science Foundation (ISF grant 2417/20), within the Israel Precision Medicine Partership program. The work of YN, AE, and KI was supported by European Research Council Consolidator Grant OCLD (project no. 681870). Senior Editor Matthias Barton, University of Zurich, Switzerland Reviewing Editor Arduino A Mangoni, Flinders Medical Centre, Australia Reviewers Francesco Pasqualini Gad Vatine, Ben Gurion University Publication history Preprint posted: March 1, 2021 (view preprint) Received: April 12, 2021 Accepted: October 9, 2021 Version of Record published: October 25, 2021 (version 1) Copyright © 2021, Rauti et al. This article is distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use and redistribution provided that the original author and source are credited. Metrics 1,400 Page views 140 Downloads 0 Citations Daily Monthly Daily Monthly Article citation count generated by polling the highest count across the following sources: Crossref, PubMed Central, Scopus. Categories and tags Research Article Microbiology and Infectious Disease SARS-COV-2 vasculature endothelium protein interactions Research organism Human The current study showed that almost 70 % (18 out of 26) of the SARS-CoV-2 proteins affect endothelial barrier integrity; however, the most significant proteins were nsp2, nsp5_c145a, and nsp7, which also induced upregulated expression of the coagulation factor VWF and cytokine release. These critical facts can shed light on the multiple pathologies observed in SARS-CoV-2 infection, including cytokine storm, increased coagulation and related diseases (e.g., heart attack and stroke) (Lee et al., 2021; Aid et al., 2020), increased cardiovascular disease, and increased neurological symptoms. The results presented here showed an effect of in vitro cultured endothelial cells, which may lead to vasculature leakiness, consequently causing exotoxicity (i.e., the penetration of toxic reagents from the blood into the brain). While there are many parameters associated with functional changes, the use of advanced tools, including network-based analysis, enabled us to elucidate the specific proteins and the specific interactions that are predicted to cause these changes. The PPI network enabled us to predict that the changes observed in barrier function are possibly due to interactions between host proteins such as cadherin 2, α-catenin, β-catenin, δ-catenin, and ZO 1 and 2, and at least with the viral proteins nsp2, nsp5_c145a, and nsp7. Moreover, we validated our PPI model performing further immunostaining analysis demonstrating not only the ability of the viral proteins to strongly impair TJ expression, but also to confirm the data predicted by our model in which some TJ proteins can be more affected than others. Coagulation AND leaky blood vessels?!?!?!?! Why haven't certain people been tried in court and hung? While beneficial, our approach has two major limitations: (a) our inability to identify the effect of multiple proteins and (b) our neglect of the effect of the coronavirus structure and binding on the cellular response. The former point can be overcome by expressing combinations of different SARS-CoV-2 proteins. However, since the SARS-CoV-2 expresses 29 proteins, there are about ~9 × 1030 possible protein combinations. Therefore, we decided to focus on individual proteins and allow further studies to pursue any combinations of interest. Regarding the latter limitation, we did not include the coronavirus structure (including the ACE2 receptors) in this study, because many studies have already demonstrated the cellular response to this structure (Chioh et al., 2020; Yang et al., 2020; Procko, 2020), and how tissues that do not have significant ACE2 expression (neurons, immune components such as B and T lymphocytes, and macrophages) are affected by the virus remains an open question. ... I'm gonna have to print this one off and read it really slow. It's not an easy read. |
|
|
|
|
[Last Edit: FlashMan-7k]
[#21]
Below are the two papers from the video.
https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(21)00648-4/fulltext https://www.thelancet.com/action/showPdf?pii=S1473-3099%2821%2900648-4 Click To View Spoiler https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3949410 https://papers.ssrn.com/sol3/Delivery.cfm/SSRN_ID3949410_code2488747.pdf?abstractid=3949410&mirid=1 Click To View Spoiler Video transcript in spoiler. Click To View Spoiler  Mandates Have Nothing To Do With Public Health so let's start here with their discussion first in the first yellow part up top quote households are the site of most sarsko v2 transmission globally in our cohort of densely sampled household contacts exposed to the delta variant sar was 30 uh that's the sars attack rate sar was 38 in unvaccinated contacts and 25 percent in fully vaccinated contacts this finding is consistent with the known protective effect of covid19 vaccination against infection it is consistent we did see that more unvaccinated contacts had a higher attack rate 38 percent so in a household somebody comes in carrying sars cov2 38 of that household if they were unvaccinated would get infected whereas it would be 25 if they were vaccinated so 38 to 25 the issue is when you look at the numbers that's not a statistically significant difference so it didn't achieve significance Also:endless boosters with a very tightly targetted vaccine (which imo isn't even possible if your natural immunity doesn't work), ... or natural immuinity that can at least recognize a slightly modified virus. Pipedream, they find a very well conserved section across a LOT of coronaviruses for a vaccine. This stupid spike-only / non sterilizing immunity stuff is biting us in the butt. conclusions for today episode 34
a current vaccines do not prevent a delta variant within households that's uk data it's just data is what it is next current vaccines drop below the 50 effectiveness barrier within 5 months for infection 6 months for severe covet that's the swedish data we also learn from that same swedish data that men the elderly and those with comorbidities are even higher risk of an early drop off in that ve the vaccine effectiveness swedish data thus the all the main logic arguments for mandates are not really found in either data or logic at this point in time the only thing we can say is that for a period of time the vaccines do prevent people from getting more serious covid and that's a good thing it's more true the effectiveness of that and the benefit of that is more true for people who are at more at risk from cove in the first place so it's a more complicated story but as you and i know the elderly and those in particular with comorbidities those are the people most at risk in this story and so the mandates then are if they're really predicated on the idea that we need the vaccine so that we can prevent the spread of covid that doesn't work anymore and if we're saying we need these vaccines because they're going to provide lasting effectiveness against severe covet and death that's not the case so we know those two things are no longer true so worse in this story for me though is that vaccinated people may falsely believe that they're safe or safer to others in society than the unvaccinated but that's not the case and so they can still transmit this disease now you might say well but on average vaccinated people are going to get a less severe course of the disease true but not completely true it's not a hundred percent true it's actually not even close to 100 true we know from the israeli data and from the uk data that the vaccinated fully vaccinated double vaccine are showing up in the hospitals and are dying that's still true so can't say it's not black and white as it's been presented it's not like you're vaccinated and safe and unvaccinated unsafe that's not the case there's risks across this whole structure so the advice here is for everybody to still keep your caution remember those four d's but particular draft and distance and the density you know being in a really uh closed air environment with a lot of other people is still risky and according to this data doesn't matter if you're vaccinated or not the only thing that really seems to matter is the younger you are the safer you seem to be and the healthier you are the safer you seem to be with one little wrinkle in there bodybuilders seem to be especially at risk from this thing it's kind of a strange thing might have something to do with their muscle mass i'm not clear about that but that data has also come through kind of anecdotally but there's too many cases there for it to be um a non-signal at this point finally but most importantly vaccines they don't deliver herd immunity they don't this is something anthony fauci should have known does know but has chosen to pretend as if he doesn't know this whole time and i've talked about that being the case right from the very beginning they can't deliver herd immunity if they don't prevent you from catching and passing on the disease it's an impossibility full stop end of story and they may vaccines may even thwart development of a more durable natural immunity because that's the end protein uk data actually we don't have data we have a statement i haven't actually seen the data yet so i'm going to go hunting for that this too deserves discussion those are my conclusions for today we should be talking about all of this what are we willing to give up what's the what are we willing to sacrifice how much are we willing to bear in order to achieve what well what are we trying to achieve |
|
|
|
|
[#22]
Originally Posted By FlashMan-7k: Why haven't certain people been tried in court and hung? Because folks are too busy driving their kids 5-11 to go get jabbed. |
|
|
|
|
[#23]
Originally Posted By exponentialpi: Because folks are too busy driving their kids 5-11 to go get jabbed. Originally Posted By exponentialpi: Originally Posted By FlashMan-7k: Why haven't certain people been tried in court and hung? Because folks are too busy driving their kids 5-11 to go get jabbed. It was a purely rehtorical question, but yeah. People who can't even look into original sources to protect their pre-teen kids to see if what they are being told is true indicates that people are ... as we humans always have been ... just buying what we want to out of what we're told. I think if you showed these people the chances of getting a case of covid as bad as having myo or peri carditis for children esp boys, vs the chances of having the same amount of damage from covid with the best data we ave ... heads would roll. |
|
|
|
|
[#24]
|
|
|
|
|
[#25]
Originally Posted By HighDesert6920: This sounds promising https://www.pfizer.com/news/press-release/press-release-detail/pfizers-novel-covid-19-oral-antiviral-treatment-candidate So, when people who took the Pfizer shots to prevent Kung Flu get a breakthru Kung Flu infection, they can take a Pfizer pill that may or may not keep them from going to the hospital or dying from the same Kung Flu that Pfizer's previous work didn't stop. These guys are milking this for all its worth. |
|
|
|
|
[#26]
Originally Posted By planemaker: So, when people who took the Pfizer shots to prevent Kung Flu get a breakthru Kung Flu infection, they can take a Pfizer pill that may or may not keep them from going to the hospital or dying from the same Kung Flu that Pfizer's previous work didn't stop. These guys are milking this for all its worth. Originally Posted By planemaker: Originally Posted By HighDesert6920: This sounds promising https://www.pfizer.com/news/press-release/press-release-detail/pfizers-novel-covid-19-oral-antiviral-treatment-candidate So, when people who took the Pfizer shots to prevent Kung Flu get a breakthru Kung Flu infection, they can take a Pfizer pill that may or may not keep them from going to the hospital or dying from the same Kung Flu that Pfizer's previous work didn't stop. These guys are milking this for all its worth. You forgot to add: They made the pfizer pill to replace other evil pills ... because those evil pills aren't profitable anymore! |
|
|
|
|
[#27]
Originally Posted By FlashMan-7k: You forgot to add: They made the pfizer pill to replace other evil pills ... because those evil pills aren't profitable anymore! Originally Posted By FlashMan-7k: Originally Posted By planemaker: Originally Posted By HighDesert6920: This sounds promising https://www.pfizer.com/news/press-release/press-release-detail/pfizers-novel-covid-19-oral-antiviral-treatment-candidate So, when people who took the Pfizer shots to prevent Kung Flu get a breakthru Kung Flu infection, they can take a Pfizer pill that may or may not keep them from going to the hospital or dying from the same Kung Flu that Pfizer's previous work didn't stop. These guys are milking this for all its worth. You forgot to add: They made the pfizer pill to replace other evil pills ... because those evil pills aren't profitable anymore! Generic drugs are evil and we must not allow them. Hope ya'll got expensive obamacare plans |
|
|
|
USA
|
[#28]
Originally Posted By HighDesert6920: This sounds promising https://www.pfizer.com/news/press-release/press-release-detail/pfizers-novel-covid-19-oral-antiviral-treatment-candidate lol |
|
|
|
[#29]
I took a look at the VAERS data today after reading the following article about "hot" lots of vaccines: Uh, That's Not A Conspiracy Theory - The Market Ticker
A few of these VAERS graphs I shared in another thread, but I made some more graphs this evening and I figured I would just share them all here in case anyone here isn't following other threads. There are a lot of graphs, so I'll put them in spoilers. First, here are some histograms of the age distribution of deaths for the vaccines, including manufacturer-specific histograms. I find it interesting that the age distributions look very similar across manufacturers. Another odd thing is that the Moderna distribution looks almost too perfect -- it peaks in the 81-85 age group and declines steadily toward younger and older age brackets, with no small peaks and valleys like the other two manufacturers. Not necessarily a sign of manipulation because it could happen by chance, but it stuck out to me. Click To View Spoiler Next, here are some different ways of looking at the numbers. These graphs below are for all manufacturers combined. The drop in deaths in the summer (June and July) corresponds to fewer doses of vaccine being distributed. However, the increase in deaths in August and September is qualitatively higher than I would have expected. Although vaccinations went up in those months, they didn't go up very much compared to summer. The last histogram in this group shows the time lag between vaccination and death. Notice that most deaths occur within 2 to 3 weeks of vaccination date. But there are some that have a much longer lag. Remember that VAERS data is unverified and there are probably some wacky entries in here. I didn't examine them enough to give a decisive opinion on the entire group. If I had a $6 billion budget like the FDA I would probably pay somebody to do that. Or maybe not. That yacht isn't going to pay off itself, amirite? Click To View Spoiler Now some scatter plots showing date of vaccination (triangles) and date of death (circles) for each manufacturer. Notice that the spread between vaccination and death starts to increase for all manufacturers after May, in an odd nonintuitive way. It's not a gradually widening spread, it just kind of diverges after May. Many deaths after May still happen shortly after vaccination, but there is a group of deaths after May for which vaccination date is April or earlier, without much in between. Again, these scatter plots look similar regardless of manufacturer. I find that very interesting. It suggests a factor that might overshadow manufacturer-specific technology or quality control. What is that factor? I don't know. Click To View Spoiler Finally, below are a couple graphs of the "hottest" Pfizer lot (EN6201) mentioned in this article: Uh, That's Not A Conspiracy Theory - The Market Ticker I also found this lot to be the "hottest" Pfizer lot, but I only counted around 40 deaths from it instead of 117 like the article says. Maybe I made a mistake. Click To View Spoiler If anyone else looks at this data, let me know what numbers you get. I did this all in Excel rather quickly, so I can't guarantee the results are error free. |
|
|
|
|
[#30]
Originally Posted By Obelix45: I took a look at the VAERS data today after reading the following article about "hot" lots of vaccines: Uh, That's Not A Conspiracy Theory - The Market Ticker A few of these VAERS graphs I shared in another thread, but I made some more graphs this evening and I figured I would just share them all here in case anyone here isn't following other threads. There are a lot of graphs, so I'll put them in spoilers. First, here are some histograms of the age distribution of deaths for the vaccines, including manufacturer-specific histograms. I find it interesting that the age distributions look very similar across manufacturers. Another odd thing is that the Moderna distribution looks almost too perfect -- it peaks in the 81-85 age group and declines steadily toward younger and older age brackets, with no small peaks and valleys like the other two manufacturers. Not necessarily a sign of manipulation because it could happen by chance, but it stuck out to me. Click To View Spoiler Next, here are some different ways of looking at the numbers. These graphs below are for all manufacturers combined. The drop in deaths in the summer (June and July) corresponds to fewer doses of vaccine being distributed. However, the increase in deaths in August and September is qualitatively higher than I would have expected. Although vaccinations went up in those months, they didn't go up very much compared to summer. The last histogram in this group shows the time lag between vaccination and death. Notice that most deaths occur within 2 to 3 weeks of vaccination date. But there are some that have a much longer lag. Remember that VAERS data is unverified and there are probably some wacky entries in here. I didn't examine them enough to give a decisive opinion on the entire group. If I had a $6 billion budget like the FDA I would probably pay somebody to do that. Or maybe not. That yacht isn't going to pay off itself, amirite? Click To View Spoiler Now some scatter plots showing date of vaccination (triangles) and date of death (circles) for each manufacturer. Notice that the spread between vaccination and death starts to increase for all manufacturers after May, in an odd nonintuitive way. It's not a gradually widening spread, it just kind of diverges after May. Many deaths after May still happen shortly after vaccination, but there is a group of deaths after May for which vaccination date is April or earlier, without much in between. Again, these scatter plots look similar regardless of manufacturer. I find that very interesting. It suggests a factor that might overshadow manufacturer-specific technology or quality control. What is that factor? I don't know. Click To View Spoiler Finally, below are a couple graphs of the "hottest" Pfizer lot (EN6201) mentioned in this article: Uh, That's Not A Conspiracy Theory - The Market Ticker I also found this lot to be the "hottest" Pfizer lot, but I only counted around 40 deaths from it instead of 117 like the article says. Maybe I made a mistake. Click To View Spoiler If anyone else looks at this data, let me know what numbers you get. I did this all in Excel rather quickly, so I can't guarantee the results are error free. The problem as I see it is you don't have the lot sizes. Without lot sizes, you can't look at actual *rates*. In theory, if you had death *rates* by lot, then you could say they are flat across lots (no QA/QC problems), normal distribution (some QA/QC problems), or disjoint (big QA/QC problems). Without having the lot sizes, you can't really compare the number of deaths directly. If one lot is 10x as large as the next, if the difference in deaths is 10x then they have the same *rate* and there really is nothing to look at relative to lots being hot or not. One other thing that is also difficult to quantify is that early on, only the elderly and those with significant co-morbidities were getting the shots. That would likely tend to skew the adverse events (particularly deaths) because of the frailty factor. So, even though Karl looked at de-coupling the age difference, there was no way to de-couple the fact that early lot numbers were given more to folks more likely to have a harsher reaction. |
|
|
|
|
[Last Edit: Obelix45]
[#31]
Originally Posted By planemaker: The problem as I see it is you don't have the lot sizes. Without lot sizes, you can't look at actual *rates*. In theory, if you had death *rates* by lot, then you could say they are flat across lots (no QA/QC problems), normal distribution (some QA/QC problems), or disjoint (big QA/QC problems). Without having the lot sizes, you can't really compare the number of deaths directly. If one lot is 10x as large as the next, if the difference in deaths is 10x then they have the same *rate* and there really is nothing to look at relative to lots being hot or not. One other thing that is also difficult to quantify is that early on, only the elderly and those with significant co-morbidities were getting the shots. That would likely tend to skew the adverse events (particularly deaths) because of the frailty factor. So, even though Karl looked at de-coupling the age difference, there was no way to de-couple the fact that early lot numbers were given more to folks more likely to have a harsher reaction. I would guess that lot size varies widely, but I really don't know. It wouldn't surprise me if they do. The "hot lot" idea needs to have a question mark for now. The thing I found interesting in the data was the similar age and time distributions of deaths between all 3 manufacturers. I was also surprised that the tail of the death distribution was still thick at lower ages, more than I would have guessed. Edited to add: The similarities between all 3 manufacturers are interesting because in my view they greatly diminish the idea that a bunch of anti vaccine crusaders are entering spurious data. If there is data manipulation, it is highly coordinated. I don't think that's happening though. My opinion for now is that most of these reports were made in good faith. |
|
|
|
|
[#32]
Originally Posted By Obelix45: I would guess that lot size varies widely, but I really don't know. It wouldn't surprise me if they do. The "hot lot" idea needs to have a question mark for now. The thing I found interesting in the data was the similar age and time distributions of deaths between all 3 manufacturers. I was also surprised that the tail of the death distribution was still thick at lower ages, more than I would have guessed. Edited to add: The similarities between all 3 manufacturers are interesting because in my view they greatly diminish the idea that a bunch of anti vaccine crusaders are entering spurious data. If there is data manipulation, it is highly coordinated. I don't think that's happening though. My opinion for now is that most of these reports were made in good faith. Originally Posted By Obelix45: Originally Posted By planemaker: The problem as I see it is you don't have the lot sizes. Without lot sizes, you can't look at actual *rates*. In theory, if you had death *rates* by lot, then you could say they are flat across lots (no QA/QC problems), normal distribution (some QA/QC problems), or disjoint (big QA/QC problems). Without having the lot sizes, you can't really compare the number of deaths directly. If one lot is 10x as large as the next, if the difference in deaths is 10x then they have the same *rate* and there really is nothing to look at relative to lots being hot or not. One other thing that is also difficult to quantify is that early on, only the elderly and those with significant co-morbidities were getting the shots. That would likely tend to skew the adverse events (particularly deaths) because of the frailty factor. So, even though Karl looked at de-coupling the age difference, there was no way to de-couple the fact that early lot numbers were given more to folks more likely to have a harsher reaction. I would guess that lot size varies widely, but I really don't know. It wouldn't surprise me if they do. The "hot lot" idea needs to have a question mark for now. The thing I found interesting in the data was the similar age and time distributions of deaths between all 3 manufacturers. I was also surprised that the tail of the death distribution was still thick at lower ages, more than I would have guessed. Edited to add: The similarities between all 3 manufacturers are interesting because in my view they greatly diminish the idea that a bunch of anti vaccine crusaders are entering spurious data. If there is data manipulation, it is highly coordinated. I don't think that's happening though. My opinion for now is that most of these reports were made in good faith. I would not have expected similar data from all 3 manufacturers. Assuming we could get rates and those, too, hold across manufacturers, then I would postulate that the problem is with the spike proteins and that we shouldn't be using any of those shots. |
|
|
|
|
[#33]
Originally Posted By Obelix45: I took a look at the VAERS data today after reading the following article about "hot" lots of vaccines: Uh, That's Not A Conspiracy Theory - The Market Ticker A few of these VAERS graphs I shared in another thread, but I made some more graphs this evening and I figured I would just share them all here in case anyone here isn't following other threads. There are a lot of graphs, so I'll put them in spoilers. First, here are some histograms of the age distribution of deaths for the vaccines, including manufacturer-specific histograms. I find it interesting that the age distributions look very similar across manufacturers. Another odd thing is that the Moderna distribution looks almost too perfect -- it peaks in the 81-85 age group and declines steadily toward younger and older age brackets, with no small peaks and valleys like the other two manufacturers. Not necessarily a sign of manipulation because it could happen by chance, but it stuck out to me. Click To View Spoiler Next, here are some different ways of looking at the numbers. These graphs below are for all manufacturers combined. The drop in deaths in the summer (June and July) corresponds to fewer doses of vaccine being distributed. However, the increase in deaths in August and September is qualitatively higher than I would have expected. Although vaccinations went up in those months, they didn't go up very much compared to summer. The last histogram in this group shows the time lag between vaccination and death. Notice that most deaths occur within 2 to 3 weeks of vaccination date. But there are some that have a much longer lag. Remember that VAERS data is unverified and there are probably some wacky entries in here. I didn't examine them enough to give a decisive opinion on the entire group. If I had a $6 billion budget like the FDA I would probably pay somebody to do that. Or maybe not. That yacht isn't going to pay off itself, amirite? Click To View Spoiler Now some scatter plots showing date of vaccination (triangles) and date of death (circles) for each manufacturer. Notice that the spread between vaccination and death starts to increase for all manufacturers after May, in an odd nonintuitive way. It's not a gradually widening spread, it just kind of diverges after May. Many deaths after May still happen shortly after vaccination, but there is a group of deaths after May for which vaccination date is April or earlier, without much in between. Again, these scatter plots look similar regardless of manufacturer. I find that very interesting. It suggests a factor that might overshadow manufacturer-specific technology or quality control. What is that factor? I don't know. Click To View Spoiler Finally, below are a couple graphs of the "hottest" Pfizer lot (EN6201) mentioned in this article: Uh, That's Not A Conspiracy Theory - The Market Ticker I also found this lot to be the "hottest" Pfizer lot, but I only counted around 40 deaths from it instead of 117 like the article says. Maybe I made a mistake. Click To View Spoiler If anyone else looks at this data, let me know what numbers you get. I did this all in Excel rather quickly, so I can't guarantee the results are error free. Great info thank you very much some things to keep in mind The shots were targeted to the elderly ( and first responders ) early on so there will be age factors in the dates also to people with significant health issues early on so that will be seen in the date data. April / May is about when it opened up to regular people in lower age groups. |
|
|
|
|
[#34]
This is a guess but I would expect lot numbers to be uniform in size. Lot numbers are manufacturing capacity batch size limited. I would expect manufacturing capacity batch size to be fairly consistent. As manufacturing capacity grew with time I would expect more lot numbers not bigger lots.
|
|
|
|
|
[Last Edit: Mach]
[#35]
the point about needing percentages not just raw numbers made by planemaker is very valid. The distribution of age would not be consistent from lot number to lot number because of the way the vax was rolled out and to who it was offered in the time variant.
|
|
|
|
|
[#36]
After my extensive reading on ADE with many other virus infections including SAR-1, MERS, HIV, etc I think there is a good chance that the difference between a mild infection and severe infection could very well be ADE during active infections.
It fits everything I have read about ADE with the other viruses and would be dependent on what type and how many of each type of antibody is made by individual immune systems. Characteristics of ADE during initial infection. 1. ADE takes hold when neutralizing antibody levels are low ( think immune system problems due to age and health) 2. sudden reversal of trend. Starting to get better then a sudden reveral to severe disease and death 3. possible cross reactivity of antibodies with previous viral infections producing ADE early on in the progression of the disease. IE rapid severe disease right from the beginning 4. Cytokine storm is an indicator of ADE and is present in severe COVD-19 infection Most of us have been saying the authorities have not been telling us something from day 1 and continue to not tell us everything. One of the key factors in ADE taking over is when neutralizing antibodies ( NaB) wane. But when they do there are still B and T cells that will make antibodies when encountering the virus . antibody waning should not make a difference with immunity and it does not in many virus and vaccine generated immunity. Yet all we hear about is needed boosters because antibodies are waning. It should not make a difference and does not make a difference with most diseases. The one type of disease that it does make a difference when antibodies wane is disease that results in ADE I am pretty much convinced we are seeing the results of ADE in people with immune systems that can not keep NaBs in production both with the infection and with the vax. I really hope I am wrong but the pieces fit including the reactions across the world by govts. I think we may be fucked hard. Yeah this is doomer shit but the ADE pieces fit the puzzle and i am saying this as someone that got vaxed because of the major brain surgery I had to have and the post viral health condition I have from either covid or lyme disease and the top doc I am going to that specializes in this says he is seeing a lot of patients with it and the long covid is very similar to chronic lyme, presents exactly the same. I feel like a deadman walking |
|
|
|
|
[#37]
Originally Posted By planemaker: So, when people who took the Pfizer shots to prevent Kung Flu get a breakthru Kung Flu infection, they can take a Pfizer pill that may or may not keep them from going to the hospital or dying from the same Kung Flu that Pfizer's previous work didn't stop. These guys are milking this for all its worth. Originally Posted By planemaker: Originally Posted By HighDesert6920: This sounds promising https://www.pfizer.com/news/press-release/press-release-detail/pfizers-novel-covid-19-oral-antiviral-treatment-candidate So, when people who took the Pfizer shots to prevent Kung Flu get a breakthru Kung Flu infection, they can take a Pfizer pill that may or may not keep them from going to the hospital or dying from the same Kung Flu that Pfizer's previous work didn't stop. These guys are milking this for all its worth. |
|
|
|
|
[#38]
Originally Posted By HighDesert6920: lol - ok, well no doubt they are milking it for all its worth financially, while the politicians milk the pandemic for all its worth in control and power grabbing....but personally, I'm glad to see treatments emerging as alternatives to the so-called vaccines... The big question though, is whether the process will be to continue with the philosophy of the individual having no say in either vaccination or treatment (vaccination is mandated, while requests for particular treatments can be denied). |
|
|
|
|
[#39]
Originally Posted By HighDesert6920: Yes, and groceries. Not necessarily for the virus so much anymore - the fomite transmission has pretty much been shown to be minimal - but for the virus and everything else. A study from several years ago (long before the chinese virus) found feces on nearly 3/4 shopping carts. Look at the people in wally world next to you....they are wiping, picking, and licking all kinds of things....the fat hairy weirdo in line ahead of you is picking his nose, swiping his greasy hair back, farts and then reaches down to scratch his ass....then goes tap, tap, tap on the payment terminal....maybe sneezes in your direction...he was rummaging through all those bags of chips just before you picked out a bag. So his nasty crotch snot is smeared across the top of your chip bag....now you've got the munchies, and open the bag of chips, rubbing your hands through that guys snot, and then you grab a handful of chips and snarf them down....infected snot and all! What about those delicious apples you enjoy? Ever drive by an apple orchard during picking season? Of course, they're all illegals - but anyway, notice where the porta-potty units are - at the edge of the field...no hand washing stations to be seen....last night was chalupa night at Dos Gringos....makes Taco Bell look like quality...the guys in the field just went there last night for cheap beer and chalupas, now they have feel a power growler coming on right before picking shift. It's a mess in there! Unfortunately no hand washing stations...so just wipe hands on pants, and start picking fresh apples for the rich gringos. Now at the store, the apples are all coated with....something...something you're going to eat - because cleaning foods before eating is for pussy doomers! You're so brave! Are you aware the the blow style hand driers in restrooms actually blow clouds of dried feces in the air every time anyone uses them? True story. |
|
|
|
|
[Last Edit: Obelix45]
[#40]
Originally Posted By Obelix45: I took a look at the VAERS data today after reading the following article about "hot" lots of vaccines: Uh, That's Not A Conspiracy Theory - The Market Ticker A few of these VAERS graphs I shared in another thread, but I made some more graphs this evening and I figured I would just share them all here in case anyone here isn't following other threads. There are a lot of graphs, so I'll put them in spoilers. First, here are some histograms of the age distribution of deaths for the vaccines, including manufacturer-specific histograms. I find it interesting that the age distributions look very similar across manufacturers. Another odd thing is that the Moderna distribution looks almost too perfect -- it peaks in the 81-85 age group and declines steadily toward younger and older age brackets, with no small peaks and valleys like the other two manufacturers. Not necessarily a sign of manipulation because it could happen by chance, but it stuck out to me. Click To View Spoiler Next, here are some different ways of looking at the numbers. These graphs below are for all manufacturers combined. The drop in deaths in the summer (June and July) corresponds to fewer doses of vaccine being distributed. However, the increase in deaths in August and September is qualitatively higher than I would have expected. Although vaccinations went up in those months, they didn't go up very much compared to summer. The last histogram in this group shows the time lag between vaccination and death. Notice that most deaths occur within 2 to 3 weeks of vaccination date. But there are some that have a much longer lag. Remember that VAERS data is unverified and there are probably some wacky entries in here. I didn't examine them enough to give a decisive opinion on the entire group. If I had a $6 billion budget like the FDA I would probably pay somebody to do that. Or maybe not. That yacht isn't going to pay off itself, amirite? Click To View Spoiler Now some scatter plots showing date of vaccination (triangles) and date of death (circles) for each manufacturer. Notice that the spread between vaccination and death starts to increase for all manufacturers after May, in an odd nonintuitive way. It's not a gradually widening spread, it just kind of diverges after May. Many deaths after May still happen shortly after vaccination, but there is a group of deaths after May for which vaccination date is April or earlier, without much in between. Again, these scatter plots look similar regardless of manufacturer. I find that very interesting. It suggests a factor that might overshadow manufacturer-specific technology or quality control. What is that factor? I don't know. Click To View Spoiler Finally, below are a couple graphs of the "hottest" Pfizer lot (EN6201) mentioned in this article: Uh, That's Not A Conspiracy Theory - The Market Ticker I also found this lot to be the "hottest" Pfizer lot, but I only counted around 40 deaths from it instead of 117 like the article says. Maybe I made a mistake. Click To View Spoiler If anyone else looks at this data, let me know what numbers you get. I did this all in Excel rather quickly, so I can't guarantee the results are error free. Ugh, I messed up when correlating the VAERS ID with manufacturers. The problem is that the VAERS data is split across three csv files, and VAERS ID is a key that can appear more than once in some files for each person. I thought I figured out how to filter it in Excel properly, but I just noticed it was incorrect. I'm going revisit this later when I have time to do something better suited to this than Excel. Anyway, the non-manufacturer specific plots should be unaffected: Click To View Spoiler |
|
|
|
|
[#41]
Originally Posted By Mach: the point about needing percentages not just raw numbers made by planemaker is very valid. The distribution of age would not be consistent from lot number to lot number because of the way the vax was rolled out and to who it was offered in the time variant. @Mach You could detect if certain lots were administered disproportionately to young or old by plotting the age distributions in the vaers data for each lot. If lot 327x was given mostly to oldsters then its distribution of adverse events should reflect that. If the lots were given randomly to all ages then the adverse events should happen similarly across ages. We know that the old have a higher vaccination rate now than the young. |
|
|
|
WV, USA
|
[#42]
Originally Posted By HighDesert6920: lol - ok, well no doubt they are milking it for all its worth financially, while the politicians milk the pandemic for all its worth in control and power grabbing....but personally, I'm glad to see treatments emerging as alternatives to the so-called vaccines... Originally Posted By HighDesert6920: Originally Posted By planemaker: Originally Posted By HighDesert6920: This sounds promising https://www.pfizer.com/news/press-release/press-release-detail/pfizers-novel-covid-19-oral-antiviral-treatment-candidate So, when people who took the Pfizer shots to prevent Kung Flu get a breakthru Kung Flu infection, they can take a Pfizer pill that may or may not keep them from going to the hospital or dying from the same Kung Flu that Pfizer's previous work didn't stop. These guys are milking this for all its worth. The pharma community, Rheumatologists, and Transplant Surgeons have known how to treat a Cytokine storm long before Covid. And since early 2020, they knew how the EXISTING drugs could effectively treat Covid as well. This whole ordeal should be an embarrassment and black eye to the entire medical community. |
|
|
|
[Last Edit: Obelix45]
[#43]
Okay, I think I'm slowly figuring out how to work with the VAERS data... I filtered it with Postgres and plotted in Excel. I only had time to look at Pfizer lot EN6201 from the Market Ticker article: Uh, That's Not A Conspiracy Theory
I also found 117 deaths associated with lot EN6201. Actually 118 because one had a blank manufacturer listing. But I just stuck with the 117 that explicitly listed Pfizer. Below are graphs of date of vax/date of death and age distribution. For context, in the spoiler, I put the symptoms listed in the "symptoms" fields for each of the 117 deaths, sorted from earliest death date to latest death date. It's a mix of sudden death, cardiac event, but also plenty of breakthrough infection deaths that happened months later. I didn't attempt to quantify any of the symptoms comments. They do show that they are not all obviously vaccine-related deaths, but some appear to be, especially the earlier entries.  Click To View Spoiler |
|
|
|
|
[#44]
Originally Posted By JHS: @Mach You could detect if certain lots were administered disproportionately to young or old by plotting the age distributions in the vaers data for each lot. If lot 327x was given mostly to oldsters then its distribution of adverse events should reflect that. If the lots were given randomly to all ages then the adverse events should happen similarly across ages. We know that the old have a higher vaccination rate now than the young. Originally Posted By JHS: Originally Posted By Mach: the point about needing percentages not just raw numbers made by planemaker is very valid. The distribution of age would not be consistent from lot number to lot number because of the way the vax was rolled out and to who it was offered in the time variant. @Mach You could detect if certain lots were administered disproportionately to young or old by plotting the age distributions in the vaers data for each lot. If lot 327x was given mostly to oldsters then its distribution of adverse events should reflect that. If the lots were given randomly to all ages then the adverse events should happen similarly across ages. We know that the old have a higher vaccination rate now than the young. One could but I can't. There is not enough data online. Looking at the lot numbers, shots from the same lot numbers are over anywhere from 2 to 6 months with no locations shown. I cross reference some of the dates that show the same lot number given out over 6 months and some of those shots were with lots that were expired. |
|
|
|
|
[#45]
Originally Posted By BlackTuono: We have a new paper to digest: https://www.mdpi.com/1999-4915/13/10/2056/htm From the journal Viruses. Synopsis - in vitro experiments have confirmed that spike proteins 1) concentrate around the nucleus in a cell 2) interfere with BRCA1 and other natural DNA repair mechanisms including 3) V(D)J recombination which is is an essential part of B and T cell development and building adaptive immunity (https://en.wikipedia.org/wiki/V) This gives a putative mechanism for two anecdotal claims that have been circulating, mainly that T cells (CD4+ and CD8 in particular) get incredibly low for some people after the second and subsequent doses, and that cancer cell activity is heightened because of the lack of immune response. In this case it isn't just the response of immune cells that is being moderated but the intracellular action to repair DNA. In case you didn't know, you all have cancer inside of you, pretty much guaranteed at any given time. Cells proliferate and encounter DNA replication errors when they split, leading to cancer eventually. Our bodies employ mechanisms to repair nicked or miscopied DNA at an intracellular level constantly. Showing that T cells can be affected is one thing, but the disruption of such a fundamental biochemical repair process is alarming when you consider we are instructing cells to churn out the spike protein itself. The authors make this point in their conclusions and propose it as a putative mechanism for some of the shot-related side effects being observed. Are we going to see a lot more cancer and AIDS-like symptoms? Hopefully not in most cases, but some people are going to get unlucky and have this effect them chronically, especially if we enter a regime where regular boosters become the norm. except the study had nothing to do with vaccine spike proteins and only virus spike proteins and it was done in vitro which means out side the body, like in a test tube. I think it is a massive jump to say if the viral spikes do something then the vaccine spikes will do it, because they are not the same. the vaccine spikes are -pre-fusion stabilized by changes in the structure. They are designed so that they can not attach to a cell. I am not saying they don't do the same thing, I am saying just because the viral spike does something doesn't mean the vax spike does it. There needs to be a follow on study with the vax spikes to know. And just because it happens in a test tube, doesn't mean in happens in a human body |
|
|
|
|
[#46]
Originally Posted By Mach: except the study had nothing to do with vaccine spike proteins and only virus spike proteins and it was done in vitro which means out side the body, like in a test tube. I think it is a massive jump to say if the viral spikes do something then the vaccine spikes will do it, because they are not the same. the vaccine spikes are -pre-fusion stabilized by changes in the structure. They are designed so that they can not attach to a cell. I am not saying they don't do the same thing, I am saying just because the viral spike does something doesn't mean the vax spike does it. There needs to be a follow on study with the vax spikes to know. And just because it happens in a test tube, doesn't mean in happens in a human body Originally Posted By Mach: Originally Posted By BlackTuono: We have a new paper to digest: https://www.mdpi.com/1999-4915/13/10/2056/htm From the journal Viruses. Synopsis - in vitro experiments have confirmed that spike proteins 1) concentrate around the nucleus in a cell 2) interfere with BRCA1 and other natural DNA repair mechanisms including 3) V(D)J recombination which is is an essential part of B and T cell development and building adaptive immunity (https://en.wikipedia.org/wiki/V) This gives a putative mechanism for two anecdotal claims that have been circulating, mainly that T cells (CD4+ and CD8 in particular) get incredibly low for some people after the second and subsequent doses, and that cancer cell activity is heightened because of the lack of immune response. In this case it isn't just the response of immune cells that is being moderated but the intracellular action to repair DNA. In case you didn't know, you all have cancer inside of you, pretty much guaranteed at any given time. Cells proliferate and encounter DNA replication errors when they split, leading to cancer eventually. Our bodies employ mechanisms to repair nicked or miscopied DNA at an intracellular level constantly. Showing that T cells can be affected is one thing, but the disruption of such a fundamental biochemical repair process is alarming when you consider we are instructing cells to churn out the spike protein itself. The authors make this point in their conclusions and propose it as a putative mechanism for some of the shot-related side effects being observed. Are we going to see a lot more cancer and AIDS-like symptoms? Hopefully not in most cases, but some people are going to get unlucky and have this effect them chronically, especially if we enter a regime where regular boosters become the norm. except the study had nothing to do with vaccine spike proteins and only virus spike proteins and it was done in vitro which means out side the body, like in a test tube. I think it is a massive jump to say if the viral spikes do something then the vaccine spikes will do it, because they are not the same. the vaccine spikes are -pre-fusion stabilized by changes in the structure. They are designed so that they can not attach to a cell. I am not saying they don't do the same thing, I am saying just because the viral spike does something doesn't mean the vax spike does it. There needs to be a follow on study with the vax spikes to know. And just because it happens in a test tube, doesn't mean in happens in a human body You do realize that in order for the spike proteins that are produced by the body after vaccination to even be worth using as a form of vaccination, the proteins produced have to be fundamentally the same as the spike protein that is on the surface of SARS-CoV-2, right? Actually, it's not fundamentally the same, it is the S protein from SARS-CoV-2 that your body produces.(ok, ok, there are changes that make your cells react stronger than they otherwise would to an S protein on SARS-CoV-2) That's the entire point of the vaccines, to prepare your body to combat the S protein. Well, the mRNA based vaccines anyways. This "the vaccine spikes are -pre-fusion stabilized by changes in the structure" is not about "They are designed so that they can not attach to a cell." The stabilization is to increase how much your body reacts to the spike protein that is produced by the mRNA. And the most effective ways to produce large amounts of viral proteins is...what viruses do, hijack the internal mechanisms of the cell to produce viral proteins. This is why the mRNA vaccines do the exact same thing. |
|
|
|
|
[Last Edit: FlashMan-7k]
[#47]
What we need is someone to test the vaccine spikes and the viral spikes to see if they behave the same way / have the same effects.
I also have beach front property in the middle of the sahara desert to sell you really cheap too.
|
|
|
|
|
[#48]
Originally Posted By HighDesert6920: This sounds promising https://www.pfizer.com/news/press-release/press-release-detail/pfizers-novel-covid-19-oral-antiviral-treatment-candidate So this should pretty much stop the need for the vax |
|
|
|
|
[#49]
Originally Posted By FlashMan-7k: What we need is someone to test the vaccine spikes and the viral spikes to see if they behave the same way / have the same effects. I also have beach front property in the middle of the sahara desert to sell you really cheap too. They do as they're functionally the same protein. |
|
|
|
|
[Last Edit: Mach]
[#50]
Originally Posted By exDefensorMilitas: You do realize that in order for the spike proteins that are produced by the body after vaccination to even be worth using as a form of vaccination, the proteins produced have to be fundamentally the same as the spike protein that is on the surface of SARS-CoV-2, right? Actually, it's not fundamentally the same, it is the S protein from SARS-CoV-2 that your body produces.(ok, ok, there are changes that make your cells react stronger than they otherwise would to an S protein on SARS-CoV-2) That's the entire point of the vaccines, to prepare your body to combat the S protein. Well, the mRNA based vaccines anyways. This "the vaccine spikes are -pre-fusion stabilized by changes in the structure" is not about "They are designed so that they can not attach to a cell." The stabilization is to increase how much your body reacts to the spike protein that is produced by the mRNA. And the most effective ways to produce large amounts of viral proteins is...what viruses do, hijack the internal mechanisms of the cell to produce viral proteins. This is why the mRNA vaccines do the exact same thing. Originally Posted By exDefensorMilitas: Originally Posted By Mach: Originally Posted By BlackTuono: We have a new paper to digest: https://www.mdpi.com/1999-4915/13/10/2056/htm From the journal Viruses. Synopsis - in vitro experiments have confirmed that spike proteins 1) concentrate around the nucleus in a cell 2) interfere with BRCA1 and other natural DNA repair mechanisms including 3) V(D)J recombination which is is an essential part of B and T cell development and building adaptive immunity (https://en.wikipedia.org/wiki/V) This gives a putative mechanism for two anecdotal claims that have been circulating, mainly that T cells (CD4+ and CD8 in particular) get incredibly low for some people after the second and subsequent doses, and that cancer cell activity is heightened because of the lack of immune response. In this case it isn't just the response of immune cells that is being moderated but the intracellular action to repair DNA. In case you didn't know, you all have cancer inside of you, pretty much guaranteed at any given time. Cells proliferate and encounter DNA replication errors when they split, leading to cancer eventually. Our bodies employ mechanisms to repair nicked or miscopied DNA at an intracellular level constantly. Showing that T cells can be affected is one thing, but the disruption of such a fundamental biochemical repair process is alarming when you consider we are instructing cells to churn out the spike protein itself. The authors make this point in their conclusions and propose it as a putative mechanism for some of the shot-related side effects being observed. Are we going to see a lot more cancer and AIDS-like symptoms? Hopefully not in most cases, but some people are going to get unlucky and have this effect them chronically, especially if we enter a regime where regular boosters become the norm. except the study had nothing to do with vaccine spike proteins and only virus spike proteins and it was done in vitro which means out side the body, like in a test tube. I think it is a massive jump to say if the viral spikes do something then the vaccine spikes will do it, because they are not the same. the vaccine spikes are -pre-fusion stabilized by changes in the structure. They are designed so that they can not attach to a cell. I am not saying they don't do the same thing, I am saying just because the viral spike does something doesn't mean the vax spike does it. There needs to be a follow on study with the vax spikes to know. And just because it happens in a test tube, doesn't mean in happens in a human body You do realize that in order for the spike proteins that are produced by the body after vaccination to even be worth using as a form of vaccination, the proteins produced have to be fundamentally the same as the spike protein that is on the surface of SARS-CoV-2, right? Actually, it's not fundamentally the same, it is the S protein from SARS-CoV-2 that your body produces.(ok, ok, there are changes that make your cells react stronger than they otherwise would to an S protein on SARS-CoV-2) That's the entire point of the vaccines, to prepare your body to combat the S protein. Well, the mRNA based vaccines anyways. This "the vaccine spikes are -pre-fusion stabilized by changes in the structure" is not about "They are designed so that they can not attach to a cell." The stabilization is to increase how much your body reacts to the spike protein that is produced by the mRNA. And the most effective ways to produce large amounts of viral proteins is...what viruses do, hijack the internal mechanisms of the cell to produce viral proteins. This is why the mRNA vaccines do the exact same thing. I spent a bunch of time researching the meaning of prefusion stabilized. Prefusion is the state of the proteins before cell attachment. Fusion is when the proteins attach to the cell wall and change their protein structure to open the cell wall to allow the viral genome into the cell. Prefusion stabilized is a change in the protein structure so the spike protein can not attach and fuse with the cell wall. It is stabilized in the prefusion form and can not change. It does result in a stronger immune response but that is because if were to fuse, lacking the other parts of the viral proteins, there would be antibodies developed that could not attack in the prefusion state. So all the antibodies made due to the vax are AB that attack the prefusion spike. https://cen.acs.org/pharmaceuticals/vaccines/tiny-tweak-behind-COVID-19/98/i38 While the spikes are fundamentally the same as the virus spikes as far as antibodies are concerned, they are not exactly the same and dont have the same functional capabilities. whether that matters in this case I dont know. There needs to be a study |
|
|
|
 Win a FREE Membership!
Win a FREE Membership!
Sign up for the ARFCOM weekly newsletter and be entered to win a free ARFCOM membership. One new winner* is announced every week!
You will receive an email every Friday morning featuring the latest chatter from the hottest topics, breaking news surrounding legislation, as well as exclusive deals only available to ARFCOM email subscribers.

AR15.COM is the world's largest firearm community and is a gathering place for firearm enthusiasts of all types.
From hunters and military members, to competition shooters and general firearm enthusiasts, we welcome anyone who values and respects the way of the firearm.

Subscribe to our monthly Newsletter to receive firearm news, product discounts from your favorite Industry Partners, and more.
Copyright © 1996-2024 AR15.COM LLC. All Rights Reserved.
Any use of this content without express written consent is prohibited.
AR15.Com reserves the right to overwrite or replace any affiliate, commercial, or monetizable links, posted by users, with our own.