|
[#1]
Gauze....don't waste your money on combat gauze....just get regular cheap gauze.....all does the same thing.....shears, tape....
If you're wanting a chest seal make sure you get a two way. Not much else is needed IMHO in an IFAK. Unless you have further medical training. |
|
|
|
[#2]
|
|
|
|
[#3]
Quoted:
Gauze....don't waste your money on combat gauze....just get regular cheap gauze.....all does the same thing.....shears, tape.... If you're wanting a chest seal make sure you get a two way. Not much else is needed IMHO in an IFAK. Unless you have further medical training. This. A couple set of gloves. (I like the way rescue essentials wraps their glove sets. An adhesive address sticker) Shears. Cat Gauze (Kerlix) 2x chest seal Israeli bandage The only other things I would suggest would be some athletic tape and some 4x4" or larger surgical pads. It's a good non-adhesive quickfix for scraped legs/knees/elbows/arms. |
|
|
|
[#4]
CAT - Do not put it in the pouch, it should stay outside easy to get to.
Combat Gauze (Chito Gauze, Celox Gauze work as well) Chest Seal (HALO - it wraps around pressure dressing really well) Olaes Pressure Dressing - 4" (better in almost every way over an Izzy and ETD) Gloves Trauma Shears Don't worry about an NPA, use positioning of the patient, lie them on their side, bend their top leg to tripod them up. Quoted:
Gauze....don't waste your money on combat gauze....just get regular cheap gauze.....all does the same thing.....shears, tape.... If you're wanting a chest seal make sure you get a two way. Not much else is needed IMHO in an IFAK. Unless you have further medical training. Sorry, but Combat Gauze has been proven to work better than regular gauze in both Quantitative Research and Qualitative Real World use. The comment that they do the same thing is like saying an stick and t-shirt will the same thing as a CAT. Maybe yes, but I would rather have the best product I can, a product made specifically for the injury. Here is a quick grab of the study done several years ago by United States Army Institute of Surgical Research (USAISR). Total Hemostasis Time - Combat Gauze doubled regular gauze. Blood loss - Combat Gauze nearly half of regular gauze. Survival Analysis - 80% over 3 hours vs. 30% over 3 hours and Combat Gauze had 100% survival out to almost 2 hours. Mean Arterial Pressure (MAP) rose and was maintained with Combat Gauze vs. a decline by every other agent. All this is dependent on proper application, so get some training in wound packing. 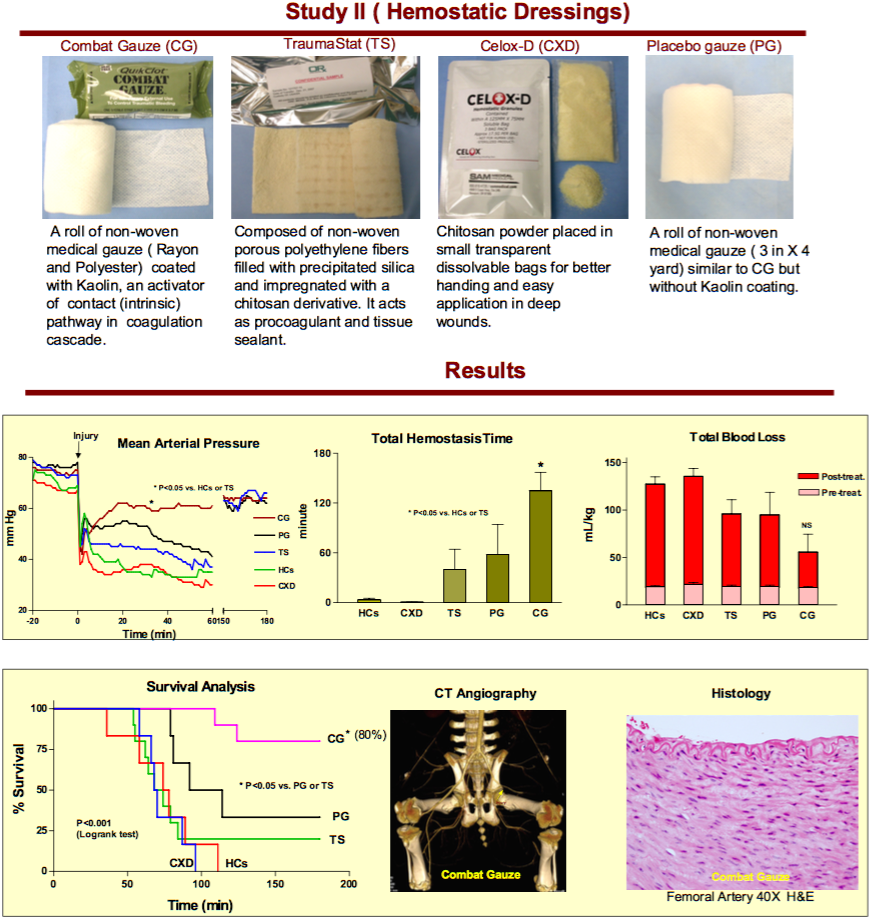
|
|
|
|
[#5]
Quoted:
So I currently am tasked with working out a policy for the carrying of small IFAKs for a relatively large set of LEOs. The kit must fit inside a pouch slightly wider and shorter than 2x AR mag pouch (2 mags are loose, but you cannot squeeze in 3). Large scale trauma care is available at several hospitals within the local area, and cost is not important for basic medical stuff, but virtually a no go for anything non standard. Current thoughts: CAT Small Israeli bandage Gloves This leaves plenty of room in the pouch, but I'm stuck with what else is needed: Combat gauze Chest seal Small shears Nasal airway Flat wrap duct tape (this is going in, but how much?) Compressed gauze Something else? Obviously, I cannot include all of these things, and in the case of either type of gauze, that would be it. Anyone have any thoughts? Assume that everyone carrying these has current TC3 training. No offense , but what is your background? If you are tasked with a Large LEO policy on IFAKS why are you coming to AR15.com for advice? There are plenty of resources available to you if a first responder- especially in Texas.....TTPOA, ALERRT, SOMA , as well as JSOMS publication. There are also plenty of agencies in Texas with Med/Ifak programs. You will get a lot of recommendations here. Some good, some old, and some that are just......Look at the current TCCC recommendations and go from there : All vetted products: TQ, trauma dressing , hemostatic gauze , vented chest seal, flat pack gauze..... |
|
|
|
[#6]
Quoted:
No offense , but what is your background? If you are tasked with a Large LEO policy on IFAKS why are you coming to AR15.com for advice? There are plenty of resources available to you if a first responder- especially in Texas.....TTPOA, ALERRT, SOMA , as well as JSOMS publication. There are also plenty of agencies in Texas with Med/Ifak programs. You will get a lot of recommendations here. Some good, some old, and some that are just......Look at the current TCCC recommendations and go from there : All vetted products: TQ, trauma dressing , hemostatic gauze , vented chest seal, flat pack gauze..... Quoted:
Quoted:
So I currently am tasked with working out a policy for the carrying of small IFAKs for a relatively large set of LEOs. The kit must fit inside a pouch slightly wider and shorter than 2x AR mag pouch (2 mags are loose, but you cannot squeeze in 3). Large scale trauma care is available at several hospitals within the local area, and cost is not important for basic medical stuff, but virtually a no go for anything non standard. Current thoughts: CAT Small Israeli bandage Gloves This leaves plenty of room in the pouch, but I'm stuck with what else is needed: Combat gauze Chest seal Small shears Nasal airway Flat wrap duct tape (this is going in, but how much?) Compressed gauze Something else? Obviously, I cannot include all of these things, and in the case of either type of gauze, that would be it. Anyone have any thoughts? Assume that everyone carrying these has current TC3 training. No offense , but what is your background? If you are tasked with a Large LEO policy on IFAKS why are you coming to AR15.com for advice? There are plenty of resources available to you if a first responder- especially in Texas.....TTPOA, ALERRT, SOMA , as well as JSOMS publication. There are also plenty of agencies in Texas with Med/Ifak programs. You will get a lot of recommendations here. Some good, some old, and some that are just......Look at the current TCCC recommendations and go from there : All vetted products: TQ, trauma dressing , hemostatic gauze , vented chest seal, flat pack gauze..... Don't worry, I am well aware of the resources available, and have a wealth of resources available for conducting actual research. As with most other things that involve getting advice/information from the Internet, the question is posed for entertainment purposes as much as anything plus the off chance someone will have an innovative way to skin the cat, as it where. |
|
|
|
[#7]
Quoted:
So I currently am tasked with working out a policy for the carrying of small IFAKs for a relatively large set of LEOs. The kit must fit inside a pouch slightly wider and shorter than 2x AR mag pouch (2 mags are loose, but you cannot squeeze in 3). Large scale trauma care is available at several hospitals within the local area, and cost is not important for basic medical stuff, but virtually a no go for anything non standard. Current thoughts: CAT Small Israeli bandage Gloves This leaves plenty of room in the pouch, but I'm stuck with what else is needed: Combat gauze Chest seal Small shears Nasal airway Flat wrap duct tape (this is going in, but how much?) Compressed gauze Something else? Obviously, I cannot include all of these things, and in the case of either type of gauze, that would be it. Anyone have any thoughts? Assume that everyone carrying these has current TC3 training. The one question to ask first: WHAT ARE YOU TRAINED TO USE?! Everything else is secondary. I can give you a whole surgical kit, but if you don't know which is the pointy end of the scalpel you aren't going to be saving anyone. Also, bear in mind when you start using medical equipment incorrectly you may be liable. EDIT Not sure what TC3 training is but when you start talking nasal airways you start thinking significant facial trauma and contraindications for placement. EDIT EDIT: Read their curriculum. Personally I would not follow it outside of BLS guidelines with the emphasis on trauma (specifically GSW). Airway placements, IVs, needle decompression, spinal injury, etc are all outside what I personally consider what regular people or those with minimal training should attempt. A lot of that, especially in a active shooter situation, is stuff that trained professional health care folks practice for months then get a lot of support when they start attempting on real people. Plus they are all skills that you will lose if you do not keep up the practice on a very regular basis. I train in a lot of that bi-yearly for ALS and NRP and I wouldn't feel super-confident darting a chest. And in today's litigious society a LEO attempting what is usually performed by a MD would definitely lead to lawsuits. Before you go past gloves and gauze I would have a very long discussion with your risk management team with lawyers for your department present making sure you are indemnified for using advanced medical equipment. |
|
|
|
[#8]
Keep it simple. You have large trauma centers very close, so you aren't trying to totally manage a patient for hours on end. Also you have to take training levels into account, but I can guess that it's not much.
So stick to a simple rule. Don't stick ANYTHING in people. A good tourniquet, CAT or SOFT-W A good pressure dressing, I prefer the Emergency Bandage, which is the new wording for the Israeli. The OALES is good, but is bulky. A good chest seal, the HALO or H&H wound closure kit are very lo-pro, stick to damn near everything, and are easy to apply. That will keep your average trauma patient alive long enough for the pros to get their hands on them. Then TRAIN your ever living asses off to make sure you can use these items effectively and quickly, otherwise you're just wasting money. |
|
|
|
[#9]
Quoted: Keep it simple. You have large trauma centers very close, so you aren't trying to totally manage a patient for hours on end. Also you have to take training levels into account, but I can guess that it's not much. So stick to a simple rule. Don't stick ANYTHING in people. A good tourniquet, CAT or SOFT-W A good pressure dressing, I prefer the Emergency Bandage, which is the new wording for the Israeli. The OALES is good, but is bulky. A good chest seal, the HALO or H&H wound closure kit are very lo-pro, stick to damn near everything, and are easy to apply. That will keep your average trauma patient alive long enough for the pros to get their hands on them. Then TRAIN your ever living asses off to make sure you can use these items effectively and quickly, otherwise you're just wasting money. |
|
|
|
[#10]
So is the Sam Med one- sticks to EVERYTHING, has easy to use tabs, and a well designed vent it cost a bit more then the others, but IMO, it's the best thing going out there
|
|
|
|
[#11]
Quoted:
The one question to ask first: WHAT ARE YOU TRAINED TO USE?! Everything else is secondary. I can give you a whole surgical kit, but if you don't know which is the pointy end of the scalpel you aren't going to be saving anyone. Also, bear in mind when you start using medical equipment incorrectly you may be liable. EDIT Not sure what TC3 training is but when you start talking nasal airways you start thinking significant facial trauma and contraindications for placement. EDIT EDIT: Read their curriculum. Personally I would not follow it outside of BLS guidelines with the emphasis on trauma (specifically GSW). Airway placements, IVs, needle decompression, spinal injury, etc are all outside what I personally consider what regular people or those with minimal training should attempt. A lot of that, especially in a active shooter situation, is stuff that trained professional health care folks practice for months then get a lot of support when they start attempting on real people. Plus they are all skills that you will lose if you do not keep up the practice on a very regular basis. I train in a lot of that bi-yearly for ALS and NRP and I wouldn't feel super-confident darting a chest. And in today's litigious society a LEO attempting what is usually performed by a MD would definitely lead to lawsuits. Before you go past gloves and gauze I would have a very long discussion with your risk management team with lawyers for your department present making sure you are indemnified for using advanced medical equipment. Quoted:
Quoted:
So I currently am tasked with working out a policy for the carrying of small IFAKs for a relatively large set of LEOs. The kit must fit inside a pouch slightly wider and shorter than 2x AR mag pouch (2 mags are loose, but you cannot squeeze in 3). Large scale trauma care is available at several hospitals within the local area, and cost is not important for basic medical stuff, but virtually a no go for anything non standard. Current thoughts: CAT Small Israeli bandage Gloves This leaves plenty of room in the pouch, but I'm stuck with what else is needed: Combat gauze Chest seal Small shears Nasal airway Flat wrap duct tape (this is going in, but how much?) Compressed gauze Something else? Obviously, I cannot include all of these things, and in the case of either type of gauze, that would be it. Anyone have any thoughts? Assume that everyone carrying these has current TC3 training. The one question to ask first: WHAT ARE YOU TRAINED TO USE?! Everything else is secondary. I can give you a whole surgical kit, but if you don't know which is the pointy end of the scalpel you aren't going to be saving anyone. Also, bear in mind when you start using medical equipment incorrectly you may be liable. EDIT Not sure what TC3 training is but when you start talking nasal airways you start thinking significant facial trauma and contraindications for placement. EDIT EDIT: Read their curriculum. Personally I would not follow it outside of BLS guidelines with the emphasis on trauma (specifically GSW). Airway placements, IVs, needle decompression, spinal injury, etc are all outside what I personally consider what regular people or those with minimal training should attempt. A lot of that, especially in a active shooter situation, is stuff that trained professional health care folks practice for months then get a lot of support when they start attempting on real people. Plus they are all skills that you will lose if you do not keep up the practice on a very regular basis. I train in a lot of that bi-yearly for ALS and NRP and I wouldn't feel super-confident darting a chest. And in today's litigious society a LEO attempting what is usually performed by a MD would definitely lead to lawsuits. Before you go past gloves and gauze I would have a very long discussion with your risk management team with lawyers for your department present making sure you are indemnified for using advanced medical equipment. If you don't know what he is referring to when he says "TC3", you should probably expand on some of your own training. He is referring to Tactical Combat Casualty Care. It's been around for about a decade now. From the rest of your post it sounds like you are a paramedic. National Registry hasn't updated much of its curriculum to cover most things in TCCC. If he is talking about having things issued to LEO, not just something they are picking up on their own, I would be willing to bet their police chief has looked into the legal ramifications. Hell, here in Maryland, some police jurisdictions are starting to carry Narcan. And not in autoinjectors either. But I digress. OP, I recently came across the Israeli T3 bandage. It's a nice option. It incorporates a second dressing pad and some z fold gauze, giving you additional bandaging capabilities. I would include the following if it were me: CAT Gloves Israeli T3 H and H compressed gauze Chest seal -Hyfin Compact twin pack is nice Nasal Airway If space permits, I like a simple 5x9 ABD pad. It's a nice additional dressing in a small package which doesn't take up much room. |
|
|
|
[#12]
So I'll expand a bit on background, since protocol seems to be giving some folks issues: this is .mil LE. So yes, everyone has medical training, it's simply a matter of moving kits out of blow out bags in the vehicle and into already available real estate on the body. And as IFAKs, these supplies are for self aid/buddy aid. There is plenty of doctrine, SOP, and real world application for other situations. Looks like we are going with:
CAT TQ stowed with the tail out. It's tight, but pulling the tail dumps the pouch. The small ETB, sans exterior packaging (a compromise for space) H&h compressed gauze - another compromise, combat gauze just can't get small enough to fit with the ETB/tourniquet. IFAK II flat rolled duct tape - not sure the length, but on hand in quantity. Gloves right on top, replaced as needed. These get used often, and where already policy. Discussion is chest seals. We want to include one, but just don't have space in the pouch. We've discussed putting them in the body armor pocket, but I can see issues with that... After all, a lot of penetrating chest trauma would pass through the vest first, posing a problem. Current thought is to push improvised seal with tape/ETB wrapper in training, and continue to drill speedy evac where possible. I'll post pics when I get the chance. |
|
|
|
[#13]
Quoted: So I'll expand a bit on background, since protocol seems to be giving some folks issues: this is .mil LE. So yes, everyone has medical training, it's simply a matter of moving kits out of blow out bags in the vehicle and into already available real estate on the body. And as IFAKs, these supplies are for self aid/buddy aid. There is plenty of doctrine, SOP, and real world application for other situations. Looks like we are going with: CAT TQ stowed with the tail out. It's tight, but pulling the tail dumps the pouch. The small ETB, sans exterior packaging (a compromise for space) H&h compressed gauze - another compromise, combat gauze just can't get small enough to fit with the ETB/tourniquet. IFAK II flat rolled duct tape - not sure the length, but on hand in quantity. Gloves right on top, replaced as needed. These get used often, and where already policy. Discussion is chest seals. We want to include one, but just don't have space in the pouch. We've discussed putting them in the body armor pocket, but I can see issues with that... After all, a lot of penetrating chest trauma would pass through the vest first, posing a problem. Current thought is to push improvised seal with tape/ETB wrapper in training, and continue to drill speedy evac where possible. I'll post pics when I get the chance. Hyfin has a compact version that is 4x4 instead if the normal 6x6 |
|
|
|
[#14]
Why not get the TQ out of the pouch and in a separate pouch on the vest - that would free up space for quick clot and a real chest seal
Big army did this with the new Ifak Another option is to look at a different pouch- one that better organizes components for quicker access of specific items as needed |
|
|
|
[#15]
OP what about something like this DA Gen 3? Looks like it fits the size requirement, you can upgrade components as you need on the order.
|
|
|
|
[#16]
Quoted:
Why not get the TQ out of the pouch and in a separate pouch on the vest - that would free up space for quick clot and a real chest seal Big army did this with the new Ifak Another option is to look at a different pouch- one that better organizes components for quicker access of specific items as needed The issue is that we have a fixed pouch layout rather than being able to just MOLLE on different pouches. The medical supplies themselves are easy, however any different nylon just isn't in the budget, leaving us with everything needing to be in the one pouch. It seems workable, for now at least, while we work some other options, which all do center around putting a TQ on the belt. |
|
|
|
[#17]
Chinook medical makes a double mag pouch IFAK card that's awesome for fitting Doc Hurleys "1st world urban center essentials" list
|
|
|
|
[#18]
Quoted:
If you don't know what he is referring to when he says "TC3", you should probably expand on some of your own training. He is referring to Tactical Combat Casualty Care. It's been around for about a decade now. From the rest of your post it sounds like you are a paramedic. National Registry hasn't updated much of its curriculum to cover most things in TCCC. If he is talking about having things issued to LEO, not just something they are picking up on their own, I would be willing to bet their police chief has looked into the legal ramifications. Hell, here in Maryland, some police jurisdictions are starting to carry Narcan. And not in autoinjectors either. But I digress. OP, I recently came across the Israeli T3 bandage. It's a nice option. It incorporates a second dressing pad and some z fold gauze, giving you additional bandaging capabilities. I would include the following if it were me: CAT Gloves Israeli T3 H and H compressed gauze Chest seal -Hyfin Compact twin pack is nice Nasal Airway If space permits, I like a simple 5x9 ABD pad. It's a nice additional dressing in a small package which doesn't take up much room. Quoted:
Quoted:
Quoted:
So I currently am tasked with working out a policy for the carrying of small IFAKs for a relatively large set of LEOs. The kit must fit inside a pouch slightly wider and shorter than 2x AR mag pouch (2 mags are loose, but you cannot squeeze in 3). Large scale trauma care is available at several hospitals within the local area, and cost is not important for basic medical stuff, but virtually a no go for anything non standard. Current thoughts: CAT Small Israeli bandage Gloves This leaves plenty of room in the pouch, but I'm stuck with what else is needed: Combat gauze Chest seal Small shears Nasal airway Flat wrap duct tape (this is going in, but how much?) Compressed gauze Something else? Obviously, I cannot include all of these things, and in the case of either type of gauze, that would be it. Anyone have any thoughts? Assume that everyone carrying these has current TC3 training. The one question to ask first: WHAT ARE YOU TRAINED TO USE?! Everything else is secondary. I can give you a whole surgical kit, but if you don't know which is the pointy end of the scalpel you aren't going to be saving anyone. Also, bear in mind when you start using medical equipment incorrectly you may be liable. EDIT Not sure what TC3 training is but when you start talking nasal airways you start thinking significant facial trauma and contraindications for placement. EDIT EDIT: Read their curriculum. Personally I would not follow it outside of BLS guidelines with the emphasis on trauma (specifically GSW). Airway placements, IVs, needle decompression, spinal injury, etc are all outside what I personally consider what regular people or those with minimal training should attempt. A lot of that, especially in a active shooter situation, is stuff that trained professional health care folks practice for months then get a lot of support when they start attempting on real people. Plus they are all skills that you will lose if you do not keep up the practice on a very regular basis. I train in a lot of that bi-yearly for ALS and NRP and I wouldn't feel super-confident darting a chest. And in today's litigious society a LEO attempting what is usually performed by a MD would definitely lead to lawsuits. Before you go past gloves and gauze I would have a very long discussion with your risk management team with lawyers for your department present making sure you are indemnified for using advanced medical equipment. If you don't know what he is referring to when he says "TC3", you should probably expand on some of your own training. He is referring to Tactical Combat Casualty Care. It's been around for about a decade now. From the rest of your post it sounds like you are a paramedic. National Registry hasn't updated much of its curriculum to cover most things in TCCC. If he is talking about having things issued to LEO, not just something they are picking up on their own, I would be willing to bet their police chief has looked into the legal ramifications. Hell, here in Maryland, some police jurisdictions are starting to carry Narcan. And not in autoinjectors either. But I digress. OP, I recently came across the Israeli T3 bandage. It's a nice option. It incorporates a second dressing pad and some z fold gauze, giving you additional bandaging capabilities. I would include the following if it were me: CAT Gloves Israeli T3 H and H compressed gauze Chest seal -Hyfin Compact twin pack is nice Nasal Airway If space permits, I like a simple 5x9 ABD pad. It's a nice additional dressing in a small package which doesn't take up much room. RT, not EMS. I said I wasn't aware of TC3 but I also checked up on it and made some edits. Narcan is going to be made OTC like the morning after pill in NY soon (if it hasn't been already). Again, pretty fucking stupid IMHO for uneducated/undereducated Joe Schmoe to start administering it (enjoy the assaults and refractory pulmonary edema). I am always very hesitant to have regular non-medical people using perishable skill tools and techniques. General rule (again, for me) is don't stick anything inside a body (NPA, needle, tubes) unless you've been taught it and been practicing it. It's not even the "can you do this on the dummy" it's the "when will you NOT do this" that really worries me. We have had people come in with overzealous field care actually killing/severely injuring the patient, which is the reason for my hesitancy. Outside of the NPA your list would work for any likely trauma. One thing I would say for a more aggressive use/carry of is C-collars but the sizing requirements unfortunately limit their widespread availability in regular settings. |
|
|
|
[#19]
WI LEO here. My agency issues a z-fold pack of hemostatic guaze and a soft TW tourniquet. Simple, easy and even the guys who slept through TCCC can pack a wound or use a TQ. Rescue is on scene almost as fast as we are in most cases and our squad cars have AED's, chest seals, and other med supplies should we need it and rescue isn't on scene or is staging down the block.
Guaze and gloves in my cargo pocket, TQ on my vest. Every new certified officer goes through TCCC as part of the WI LESB curriculum. |
|
|
|
[#20]
Quoted:
RT, not EMS. I said I wasn't aware of TC3 but I also checked up on it and made some edits. Narcan is going to be made OTC like the morning after pill in NY soon (if it hasn't been already). Again, pretty fucking stupid IMHO for uneducated/undereducated Joe Schmoe to start administering it (enjoy the assaults and refractory pulmonary edema). I am always very hesitant to have regular non-medical people using perishable skill tools and techniques. General rule (again, for me) is don't stick anything inside a body (NPA, needle, tubes) unless you've been taught it and been practicing it. It's not even the "can you do this on the dummy" it's the "when will you NOT do this" that really worries me. We have had people come in with overzealous field care actually killing/severely injuring the patient, which is the reason for my hesitancy. Outside of the NPA your list would work for any likely trauma. One thing I would say for a more aggressive use/carry of is C-collars but the sizing requirements unfortunately limit their widespread availability in regular settings. Quoted:
Quoted:
Quoted:
Quoted:
So I currently am tasked with working out a policy for the carrying of small IFAKs for a relatively large set of LEOs. The kit must fit inside a pouch slightly wider and shorter than 2x AR mag pouch (2 mags are loose, but you cannot squeeze in 3). Large scale trauma care is available at several hospitals within the local area, and cost is not important for basic medical stuff, but virtually a no go for anything non standard. Current thoughts: CAT Small Israeli bandage Gloves This leaves plenty of room in the pouch, but I'm stuck with what else is needed: Combat gauze Chest seal Small shears Nasal airway Flat wrap duct tape (this is going in, but how much?) Compressed gauze Something else? Obviously, I cannot include all of these things, and in the case of either type of gauze, that would be it. Anyone have any thoughts? Assume that everyone carrying these has current TC3 training. The one question to ask first: WHAT ARE YOU TRAINED TO USE?! Everything else is secondary. I can give you a whole surgical kit, but if you don't know which is the pointy end of the scalpel you aren't going to be saving anyone. Also, bear in mind when you start using medical equipment incorrectly you may be liable. EDIT Not sure what TC3 training is but when you start talking nasal airways you start thinking significant facial trauma and contraindications for placement. EDIT EDIT: Read their curriculum. Personally I would not follow it outside of BLS guidelines with the emphasis on trauma (specifically GSW). Airway placements, IVs, needle decompression, spinal injury, etc are all outside what I personally consider what regular people or those with minimal training should attempt. A lot of that, especially in a active shooter situation, is stuff that trained professional health care folks practice for months then get a lot of support when they start attempting on real people. Plus they are all skills that you will lose if you do not keep up the practice on a very regular basis. I train in a lot of that bi-yearly for ALS and NRP and I wouldn't feel super-confident darting a chest. And in today's litigious society a LEO attempting what is usually performed by a MD would definitely lead to lawsuits. Before you go past gloves and gauze I would have a very long discussion with your risk management team with lawyers for your department present making sure you are indemnified for using advanced medical equipment. If you don't know what he is referring to when he says "TC3", you should probably expand on some of your own training. He is referring to Tactical Combat Casualty Care. It's been around for about a decade now. From the rest of your post it sounds like you are a paramedic. National Registry hasn't updated much of its curriculum to cover most things in TCCC. If he is talking about having things issued to LEO, not just something they are picking up on their own, I would be willing to bet their police chief has looked into the legal ramifications. Hell, here in Maryland, some police jurisdictions are starting to carry Narcan. And not in autoinjectors either. But I digress. OP, I recently came across the Israeli T3 bandage. It's a nice option. It incorporates a second dressing pad and some z fold gauze, giving you additional bandaging capabilities. I would include the following if it were me: CAT Gloves Israeli T3 H and H compressed gauze Chest seal -Hyfin Compact twin pack is nice Nasal Airway If space permits, I like a simple 5x9 ABD pad. It's a nice additional dressing in a small package which doesn't take up much room. RT, not EMS. I said I wasn't aware of TC3 but I also checked up on it and made some edits. Narcan is going to be made OTC like the morning after pill in NY soon (if it hasn't been already). Again, pretty fucking stupid IMHO for uneducated/undereducated Joe Schmoe to start administering it (enjoy the assaults and refractory pulmonary edema). I am always very hesitant to have regular non-medical people using perishable skill tools and techniques. General rule (again, for me) is don't stick anything inside a body (NPA, needle, tubes) unless you've been taught it and been practicing it. It's not even the "can you do this on the dummy" it's the "when will you NOT do this" that really worries me. We have had people come in with overzealous field care actually killing/severely injuring the patient, which is the reason for my hesitancy. Outside of the NPA your list would work for any likely trauma. One thing I would say for a more aggressive use/carry of is C-collars but the sizing requirements unfortunately limit their widespread availability in regular settings. RT? Respiratory Therapist? Radiology Tech? Just curious how it relates to your experience in the field of trauma care. I agree with you that people who arent trained properly shouldn't be sticking things into people that they arent fully trained with. While I am ok with most basic trained people with NPAs, I DO NOT like chest darts. Most people who need to be decompressed have some time before it becomes an issue. But it is not a an immediate treatment that is required. And as far as cervical collars, 1) adjustable sizing collars are readily available and have done away with the need for carrying a set of different sizes, and 2) most studies haveshown that they arent really necessary in *most* situations. As a matter of fact full spinal immobilization, which was once the norm for just about everything (including penetrating trauma to the torso) has been proven to do more harm than good. |
|
|
 Win a FREE Membership!
Win a FREE Membership!
Sign up for the ARFCOM weekly newsletter and be entered to win a free ARFCOM membership. One new winner* is announced every week!
You will receive an email every Friday morning featuring the latest chatter from the hottest topics, breaking news surrounding legislation, as well as exclusive deals only available to ARFCOM email subscribers.

AR15.COM is the world's largest firearm community and is a gathering place for firearm enthusiasts of all types.
From hunters and military members, to competition shooters and general firearm enthusiasts, we welcome anyone who values and respects the way of the firearm.

Subscribe to our monthly Newsletter to receive firearm news, product discounts from your favorite Industry Partners, and more.
Copyright © 1996-2024 AR15.COM LLC. All Rights Reserved.
Any use of this content without express written consent is prohibited.
AR15.Com reserves the right to overwrite or replace any affiliate, commercial, or monetizable links, posted by users, with our own.








